The SARS CoV-2, a mutated sub-microscopic agent
lacking a true existence of its own, has brought the world to a
standstill (literally and metaphorically). Several countries
have gone in to a complete lock-down to limit the spread of the
Coronavirus disease 2019 (COVID-19) pandemic. The primary focus
has rightly been on curbing the disease spread in the community,
rapid development and re-organization of available medical
resources to cater to the increasing patient load and adequate
care of the infected ones. Most other things have taken a
backseat. Education at all levels has become uncertain due to
the mass closures of schools and universities. Medical
education, particularly, at the medical school/undergraduate
level, has been no exception.
HOW HAS MEDICAL EDUCATION BEEN AFFECTED?
The premise for closing medical universities is dual – medical
students’ safety may be jeopardized during clinical rotations
putting them at risk of exposure to COVID-19 positive patients,
and/or infected students may themselves become the portal of
spread of the disease [1]. Even for preclinical medical
students, social distancing measures have precluded the conduct
of classroom-based teaching and discussions [2]. In the wake of
this global emergency, medical education has been existentially
challenged.
In certain countries like the US, the pandemic has
coincided with the time of educational transition [3]. A steep
rise in the infection rates has forced a complete removal of the
students from the clinical rotations [4] and halting of all
summative examinations. Several Canadian, UK and Australian
schools have taken similar urgent steps [5,6]. As a result,
scores of medical students have been affected with final year
medical students stuck just short of graduation.
In countries like India, where the educational transition
has already occurred, the current clinical rotations have been
halted. A particular concern is the implementation of the new
competency-based curriculum for the students admitted in 2019.
Almost all the institutions in the country had put up a
day-by-day time table covering the entire phase 1, which is
going to be disrupted. Additionally, it was about the time to
prepare for the phase 2 in terms of objectives, integration and
preparing schedules. Teachers of phase 2 also needed training
for the new curriculum. This process has been paused. Medical
students (admitted both pre-2019 and post-2019) will suffer a
reduced exposure to certain clinical branches or a
proportionally shortened rotation in all clinical branches. In
the worst-case scenario, where the pandemic continues for an
unforeseeable time, an extension of the medical training period
may be warranted. In all situations, the medical students will
be at a loss.
Thus, the medical educators need to rapidly evolve
the methods of teaching to minimize the onslaught of disrupted
medical education, while also building innovative systems to
accommodate the medical student cohorts stuck in the time of
this pandemic. Medical Council of India has come out with its
guidance for medical students in the current situation [7].
WHY SHOULD MEDICAL EDUCATION CONTINUE?
There are three important reasons for ensuring continuation of
medical education in this hour. Firstly, learning the science
and art of medicine is a graduated process, it is imperative
that a student completes one milestone before embarking on the
next. A student who misses any part of the education is likely
to find it difficult to join the dots later. Secondly, if
clinical rotations are deferred for the current student cohort
and clubbed with others, the density of learners would impair
the clinical learning experience (especially in geographic areas
like India where the learner density is already very high).
Lastly, recognizing the possibility that the current pandemic
may take a reasonable time to abate, there may arise a paucity
of healthcare workers. In such situations, students may need to
engage in certain aspects of patient care while the authorities
ensure their safety, learning and if applicable, remuneration.
Therefore, it is essential that we adopt new ways
that facilitate the ongoing knowledge and skill development of
the next generation of health professionals.
MAINTAINING THE CONTINUITY OF MEDICAL EDUCATION
To answer this, we may first reiterate that undergraduate
medical education the world over is divided into an initial
foundation of preclinical teaching (lasting 12-24 months)
followed by the core of clinical rotations or clerkships
(lasting 24 months) in medical schools following the
conventional model [1]. This is followed by internship where the
student works with the treating team as a supervised learner.
Finally, as per the concerned university’s regulations, the
medical student applies for/appears for entrance exams to
specialized courses (residency or post-graduation) during the
final year of medical school or during internship.
Conventionally, the preclinical teachings have
involved lectures, small group discussions and laboratory
sessions. For the past decade, the medical fraternity has been
trying to improvise pedagogy by introducing technology-based
novel concepts such as flipped lectures and simulation-based
learning [8,9]. Though, many medical schools have become well
versed with these concepts, in several countries including
India, technology-enhanced learning is still in its infancy. In
wake of the COVID-19 pandemic, a number of medical schools have
rapidly converted their entire pre-clinical curriculum to online
formats involving online lectures, webcasting and virtual group
discussions. However, such transition may be slower in places
where technology enhanced learning is still developing and
online lectures still need to be prepared, especially when a
large part of the medical fraternity has been redirected to
fight the COVID-19 pandemic. While enforcement of
technology-based learning has become a necessity in this hour,
we need to ponder upon the advantages and barriers it may pose.
Online formats allow the students an easy accessibility to
educational material as per their convenience, in their
preferred environments and repeatedly. Pitfalls include
isolation due to shifting from the medical school setting to
home, reduced discussions with peers, increased dependence on
email and an uninterrupted internet access, and a struggle to
delineate boundaries between work and home [1]. There have been
instances of many medical schools in India having started online
lectures for students; however, most of these are conventional
lectures delivered through electronic mode, without paying much
attention to the pedagogical requirements of online learning.
Additionally, very few have incorporated the assessment
component in these.
Clinical teachings, on the other hand are best learnt bedside
with a ‘live’ patient. Not only does the medical student get a
first-hand experience of patient’s clinical findings but also
learns about the dynamics of patient interaction, psychology and
counselling. In addition, development of a student’s
professional identity is often shaped by medical teachers who
they see as role models and who can infuse the cultures of
altruism. However, in the times of this contagious pandemic, an
alternate model is needed wherein some form of clinical
education continues despite curtailment of
real patient contact. Cues can be taken from the past.
During the SARS outbreak which preferentially affected the
healthcare workers [10], an infection of 17 medical students
provoked rapid closure of the Chinese university in Honk Kong in
2003 [11]. This period saw heavy reliance on technology-based
learning to provide some continuum to clinical teaching. These
included webcasting, videotaped vignettes, audio-recordings,
problem-based learning tutorials on online chat rooms and
mannequin simulators [11,12]. Over the years, technology has
matured. The current situation demands use and furthering of
these pedagogical innovations. Use of e-learning modules (flash
multimedia and digitized images), patient surrogates such as
virtual patients (to teach clinical examination, procedural,
diagnostic skills and communication skills) and virtual-reality
simulators (to teach palpation, surgical and resuscitation
skills) is needed. Simulators have shown to be as effective as
live actor-patients for teaching purposes [13]. Despite the
undoubted advantage of IT and simulation-based education, in the
current situation, there are distinct disadvantages. The
foremost is the fact that all these tools can be supplemental to
clinical teaching but not a replacement. Secondly, setting up of
a virtual learning environment or a simulation laboratory is
costly and time taking, making it especially unsuited for the
low and middle income countries. Thirdly, while virtual
simulators will maintain the tenet of both non-contact with
patient and social distancing amongst students, mannequin
simulators will flout social distancing needs amongst students
precluding their use currently.
Other important barriers that have prevented medical educators
to dissipate e-teaching (during these emergent times and
otherwise) include time constraints, poor technical skills,
inadequate infrastructure and absence of institutional
strategies. Proposed solutions include improved educator skills
(which may not be feasible in the short-term, therefore tagging
with people who already have these skills may help), inculcation
of a positive attitude, and incentives/ reward for the time
devoted to the development and delivery of online content [14].
While it may appear impressive to talk about
online/digital/simulation-based learning, the fact remains that
in India, we are still far away from such modalities [15]. It
requires planning, trained manpower and finances to embark upon
such methods. In such times, it may be very useful to have a
central agency (like MCI) to take the lead and develop
pedagogically useful learning content. A mandatory component of
formative assessment also needs to be included to ensure
attainment of learning objectives. Having a common curriculum
and rotation schedule for all colleges of India could prove to
be a blessing in disguise, allowing us to have centrally
prepared material. Many colleges in the public sector and some
in private sector have good equipment which can be put to use.
Availability of scattered expertise across institutions can be
collated for better results. There have been some recent
publications from India to highlight the role of social media as
a tool for engaging students [16,17]. Similarly, existing
professional networks can be used for webinars on important
topics.
Last year, the MCI had embarked on a digital project to monitor
teaching in colleges using closed-circuit television (CCTV)
cameras and currently most colleges have such systems in place
[18]. This infrastructure can be put to reverse use by streaming
content from MCI to all colleges, which can subsequently be
accessed by students by logging on to their institutional
servers.
In addition to the use of above tools, there may be a few
measures that may smartly squeeze some moments of clinical
learning for the medical students. These include modification of
the academic roster (preponing scholarly work and deferring
clinical rotations to a later time frame) which may be feasible
at certain medical centers as per their learning goals. Also,
students may be involved in the tele-health consultations (which
have become far commoner during this pandemic). Most
importantly, they may serve as educators to their peers,
patients and communities by developing educational materials and
videos, thus influencing behaviors in a positive way to prevent
the spread of the pandemic. Students may update themselves with
authentic online resource related to the COVID-19 pandemic;
learn via following the pandemic trajectory worldwide and
understanding how the situations are being dealt. With updated
knowledge, they may engage in projects involving development of
videos (eg, videos demonstrating donning and doffing of
PPE, proper mask fitting and hand washing techniques) or help in
preparing indigenous PPE, in the process educating themselves.
No number of lectures can match the impact of things learnt
via first-hand experience of the SARS-Cov-2 pandemic.
As far as the postgraduate students are concerned, they have
been deployed as a part of COVID workforce, their work areas
defined as per their specialization subject and year of ongoing
post-graduation. An infodemic of COVID-19 has flooded the social
and news media. It is the medical educators’ role to provide the
residents with the most reliable and latest information from the
official government and hospital websites. Repeated training
regarding PPE, donning and doffing, COVID-19 sampling, patient
handling, transport and treatment is being conducted via
online reading material, videos, webinars and cloud computing
platforms (Like Zoom, G Suite, Office 365). While the resident
teams on duty are engaged in active learning of COVID-19, those
who are in quarantine/ reserve teams may participate in
self-directed online group discussions on other important topics
of their specialty. Medical educators may guide in
identification of these topics and moderate such discussions.
Case vignettes may be presented and discussed. Many e-learning
activities are already being conducted, albeit a formative
assessment component needs to be integrated into the framework.
Thus, the options are continually evolving.
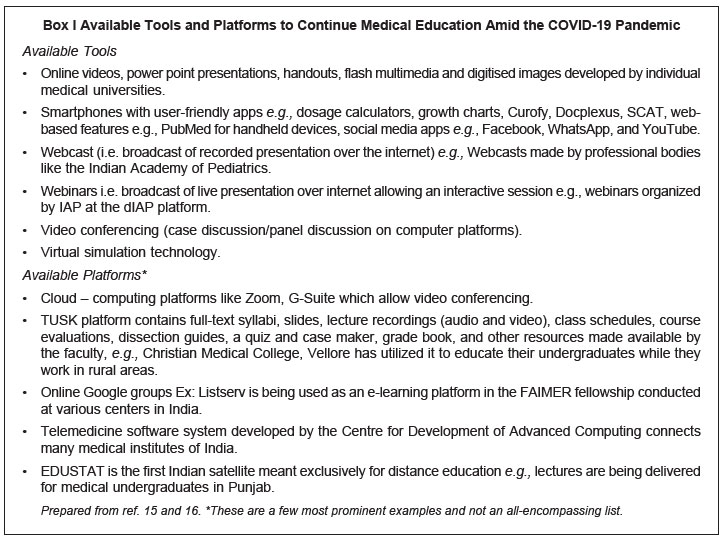
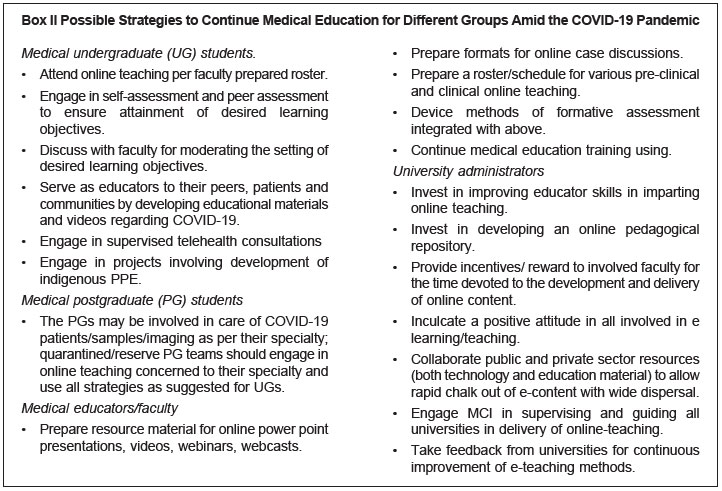
Box I shows the various available tools while
Box II enlists the various possible strategies that
may be used for continuing medical education in these times in
the Indian set-up. The most reasonable strategy will be for
every medical school to model continued pre-clinical and
clinical teachings to match with the available resources.
METHODS OF ASSESSMENT AND LICENSURE
In medical universities, where students were in the phase of
transition to the next years, examinations have been delayed.
For example, in the US, the second and third year undergraduate
summative examinations have been put on hold and the
organization that operates these testing centers has temporarily
closed its facilities [3]. Such delays are demotivating for the
exam-going students and may put their career path on the back
foot, if the closures extend. In universities where the final
year medical students have been selected for a residency, early
graduation should be considered a viable option. The medical
education systems are already emphasizing the need for
achievement of core competencies rather than mere completion of
a stipulated time period in a subject. Therefore, in these
pressing times, it may be suitable to give leeway to medical
universities to decide which medical students have completed the
necessary competencies for graduating to the next level, as
already done in the US [5]. This will not only provide a boost
to the students but also add to the healthcare work-force, who
can step up per the demands of the situation. In India, the same
situation of transition applies to the final year residents who
are at the cusp of their post-graduation. The MCI has directed
them to continue working in their respective universities to add
to the anti-COVID workforce. An early post-graduation for these
residents based on sturdy assessment merits a thought. An
internal committee may be formed by MCI to decide criteria for
eligibility for such an expedited degree.
Nevertheless, an important point to contemplate is
the method of summative assessment to be employed while
maintaining social distancing. In the past, during the SARS
outbreak in 2003, the summative examinations at certain
universities were conducted via telephone
conference-based viva voice [11]. Though, it is subject to
availability of an uninterrupted internet access, it may be
feasible in dire situations. Supplemental methods may involve
online web-based clinical case viva, demonstration of practical
skills on virtual mannequins and use of digitized images for
spotters. In a routine situation, these methods of assessment
would sound very odd, but we are living in extraordinary times
demanding extraordinary measures. In India, most undergraduates
are in the second quarter of their respective academic years and
have a long way to go before appearing for their summative
examinations. However, whether the ongoing technology-based
teaching efforts/ self-learning efforts are leading to
fulfillment of desired learning objectives is a definite
concern. Formative assessments should therefore be integral to
such efforts. Using either existing quizzes apps or indigenously
developed ones can be shared amongst institutions for this
purpose. Gamification is another upcoming modality; though, it
will need time to be cultivated. Meanwhile, self-assessment and
peer assessment are methods which may be suited to current
situation and may be encouraged while educators moderate this
process.
PLAN FOR THE FUTURE
A solid take away from the situation that we face today is that
we need to prepare for continuing medical education, not only
for now but also for possible future contagions. An excellent
approach to continuing teaching and training in medical
education field was published a decade back based on whether
only patient-student contact is to be curtailed or all forms of
contact (patient-student, student-student, teacher-student) need
to be disrupted [19]. The ongoing pandemic has already put
resource development for continuing education on a fast track.
However, it will be reasonable to invest in these pedagogical
innovations over the long-term and develop a repository of the
requisite sources beforehand.It may also be the right time to
prepare a plan B for future exigencies by involving regulators,
universities, educational experts and professional associations.
CONCLUSIONS
How do we choose to see the glass: half full or half empty? Our
optimist’s mind tells us that this period of ‘no teaching’ can
be the period of ‘greatest learning’. Medical students are
watching first-hand the principles of epidemiology in practice
and are more aware of the dynamics of a pandemic, use of PPE,
and importance of hand hygiene. Additionally, many students have
the time now to catch up on their previous studies. Medical
educators have been provided with the perfect opportunity to
develop and evaluate the suitability and application of
technology-based learning. Medical regulatory bodies and
associations have the most important reason to connect and
integrate education materials and methodologies. And humanity
has rediscovered the value of enjoying the little things in
life!
Pedagogically speaking, this time is likely to
bring out medical ingenuity. Whether online teaching becomes a
standard mode of pre-clinical education, and virtual and
simulation technology an integral part of clinical education is
for time to see, but the seeds for a paradigm shift already seem
to be have been sown.
Contributors:
PKS: Reviewed literature, drafted the manuscript; DM: concept,
manuscript plan, and inputs in manuscript preparation; TS:
contributed to manuscript planning, and provided critical inputs
in preparation and finalization.
Funding:
None; Competing interest: None stated.
REFERENCES
1.
Rose S. Medical student education in the time of
COVID-19. JAMA. March 31, 2020. Available https://www.ncbi.
nlm.nih.gov/pubmed/32232420. Accessed April 1, 2020.
2.
Del Rio C, Malani PN. 2019 Novel coronavirus – Important
information for clinicians. JAMA. February 5, 2020. Available
from: https://www.ncbi.nlm.nih.gov/pubmed/32022836.
Accessed April 1, 2020.
3.
Murphy B. Four questions medical students are asking on
the COVID-19 pandemic. Public Hlth. 2020 March 24. Available
from:
https://www.ama-assn.org/delivering-care/public-health/4-questions-medical-students-are-asking-covid-19-pandemic.
Accessed April 1, 2020.
4.
Association of American Medical Colleges. Important
guidance for medical students on clinical rotations during the
coronavirus (COVID-19) outbreak. Press release. (Published March
17, 2020). Available from:
https://www.aamc.org/news-insights/press-releases/important
guidance-medical-students-clinical-rotationsduring-coronavirus-covid-19-outbreak.
Accessed April 1, 2020.
5.
Liaison Committee on Medical Education. COVID-19 up-dates
and resources. (Updated March 25, 2020). Available from:
https://lcme.org/covid-19/. Accessed April 1, 2020.
6.
Medical Schools Council. Information for medical
students. Updated March 13, 2020. Available from:https://www.gmc-uk.org/news/news-archive/coronavirus-information-and-advice/information-for-medical-students.
Accessed April 8, 2020.
7.
Medical Council of India. Advisory regarding UG classes
in view of COVID-19 epidemic. Medical Council of India.
Published March 23, 2020. Available from: https://
mciindia.org/MCIRest/open/getDocument?path=/Documents/Public/Portal/
LatestNews/ Advisory-COVID-19-all%20colleges.pdf. Accessed
on April 8, 2020.
8.
Irby DM, Cooke M, O’Brien BC. Calls for reform of medical
education by the Carnegie foundation for the advancement of
teaching: 1910 and 2010. Acad Med. 2010;85:220-7.
9.
Skochelak SE, Stack SJ. Creating the medical schools of
the future. Acad Med. 2017;92:16-9.
10.
Maunder RG, Lancee WJ, Balderson KE, Bennett JP,
Borgundvaag B, Evans S, et al. Long-term psychological
and occupational effects of providing hospital healthcare during
SARS outbreak. Emerg Infect Dis. 2006;12:
1924-32.
11.
Patil NG, Chan Y, Yan H. SARS and its effect on medical
education in Hong Kong. Med Educ. 2003;37:1127-8.
12.
Abrahamson SD, Canzian S, Brunet F. Using simulation for
training and to change protocol during the outbreak of severe
acute respiratory syndrome. Crit Care. 2006;10:R3.
13.
Gillett B, Peckler B, Sinert R, Onkst C, Nabors S, Issley
S, et al. Simulation in a disaster drill: Comparison of
high-fidelity simulators versus trained actors. Acad Emerg Med.
2008;15:1144-51.
14.
O’Doherty D, Dromey M, Lougheed J, Hannigan A, Last J,
McGrath D. Barriers and solutions to online learning in medical
education - An integrative review. BMC Med Educ. 2018;18:130.
15.
Dhir SK, Verma D, Batta M, Mishra D. E-learning in
medical education in India. Indian Pediatr. 2017;54:871-7.
16.
Kapoor A, Tiwari V, Kapoor A. Teaching undergraduates
beyond the classroom: Use of WhatsApp. Indian Pediatr.
2019;56:967-9.
17.
Raiman L, Antbring R, Mahmood A. WhatsApp messenger as a
tool to supplement medical education for medical students on
clinical attachment. BMC Med Educ. 2017; 17:7.
18.
Medical Council of India. Implementation of IP based CCTV
solutions at Medical Colleges (DMMP-II) – Reg. April 12, 2019.
Available from:
https://mciindia.org/MCIRest/open/getDocument?path=/Documents/Public/Portal/LatestNews/Letter-all-college-DMMP-II-01.03.2019-min_compressed.pdf.
Accessed April 8, 2020.
19.
Lim E CH, Oh V MS, Koh DR, Seet R CS. the challenges of
“continuing medical education” in a pandemic era. Ann Acad Med
Singapore.2009;38:724-6.