Autoinflammatory diseases are a group of disorders characterized
by unprovoked, recurrent, sterile inflammation episodes [1], the
various conditions reported include Familial Mediterranean fever
(FMF), Tumor necrosis factor receptor associated periodic fever
syndrome (TRAPS), Mevalonate kinase deficiency (MKD). FMF is the
most encountered AIDs caused by mutation in MEFV,
characterized by recurrent fever, serositis, arthralgia or
arthritis [1,2]. TRAPS is caused by autosomal dominant mutations
in TNFRSF1A. The clinical features include recurrent
fever, abdominal pain, pleuritis, myalgias, arthralgias,
periorbital edema, and conjunctivitis. Mevalonate kinase
deficiency (MKD) is a rare disorder caused by mutations in
MVK. The clinical features of MKD are early onset of
recurrent fever episodes accompanied by lymphadenopathy,
erythematous skin rashes, hepatomegaly, splenomegaly, arthritis,
and gastrointestinal symptoms [3]. Auto-inflammatory diseases
are disorders of the innate immune system results in
overproduction of proinflammatory cytokines, including IL-1b [2]. FMF, MKD, and TRAPS are classified in IL-1–mediated
diseases [1]. IL-1 blocking agents, including canakinumab, an
anti-IL-1b monoclonal antibody, have been approved for the treatment of
these diseases [2,4-6].
Growth parameters are well-known
indicators of a child well-being that mostly affected in
children with chronic inflammatory diseases or autoinflammatory
[7-9]. Although, there are several reports on effect of
colchicine on growth parameters of FMF [8,10,11], to our
knowledge the effects of canakinumab on growth parameters of
autoinflammatory diseases have not been investigated so far.
Methods
This study had a
retrospective design and included colchicine resistant FMF, MKD,
TRAPS, and deficiency of ADA2 (DADA2) patients, treated with
canakinumab for at least six consecutive months. All patients
were diagnosed and followed by a same pediatric rheumatologist
in our tertiary referral center. FMF patients were diagnosed
according to Tel Hashomer Diagnostic criteria [12] and diagnosis
were supported by MEFV analysis. Colchicine-resistant
patients were defined according to Turkish FMF study group [13].
Disease activity of patients with FMF, MKD and TRAPS were
calculated retrospectively before and after canakinumab by using
the Autoinflammatory Diseases Activity Index (AIDAI) [14].
Diagnosis of MKD was confirmed by
genetic analysis and the patients with bi-allelic mutations in
MVK were considered as MKD. TRAPS patients were diagnosed
according to the genetic analyzes of TNFRSF1A. The
diagnosis of DADA2 was confirmed by mutations in CECR1.
We utilized the MEFV, MVK, TNFRSF1A, and CECR1
analysis as molecular diagnostics tools by using a
next-generation sequencing platform (MiSeq System, Illumina, San
Diego, CA, USA).
Demographic parameters, including
age, gender, clinical manifestations, medical data of the
patients were retrospectively obtained from medical files.
Complete blood count, acute phase reactants (APRs), including
erythrocyte sedimentation rate (ESR) and C-reactive protein
(CRP), studied before and after canakinumab administration were
also collected from medical files.
Growth parameters, including weight,
height, and BMI were recorded. Height (cm) and weight (kg) were
preferentially measured in the morning at each visit by the same
operator with the same type of stadiometer (Harpender). Standard
deviation (SD) scores of growth parameters were calculated by
anthropometric references in Turkish children [15]. The study
protocol was approved by local Ethics Committee. Written
informed consent was obtained from legal guardians of each
patient before the study.
Statistical
analysis:
The SPSS 20.0 statistical software (IBM SPSS Statistics) was
utilized. Kolmogorov-Smirnov test, stem-and-leaf diagram, and
the histogram was utilized for the confirming the normality of
distribution of growth indices. Paired-sample t-test was used
for comparing two dependent variables in the same study group
and Wilcoxon signed rank test was used for two independent
variables. The statistical level of significance for all tests
was considered to be 0.05.
Results
Totally 24 patients (13 males) with auto-inflammatory diseases
were included to the study. Eleven (45.8%) patients had
diagnosis of FMF, 9 had MKD, 3 had TRAPS, and one had DADA2.
Present study also contains the data of 10 patients reported in
the previous study [16], whose growth parameters were available.
A girl patient had a Met694Val/null mutation in MEFV
besides the diagnosis of DADA2, which was reported previously,
elsewhere [3]. The median age at diagnosis was 6.06 (range,
1.45-16.06) years. The mean age at study time was 11.29±5.21
years. The median diagnostic delay was 2.67 years (0.24-15.56).
The median age at canakinumab initiation was 9.72 (range,
1.82-19.11) years, and median follow-up during treatment was
1.59 (range, 0.56-4.33) years; and the median dose used was 10
(4-27) doses.
Patients with FMF had recurrent
fever attacks accompanying with abdominal pain, increased APRs
and were given colchicine together with canakinumab. One of the
FMF patients also had polyarticular chronic arthritis which were
treated unsuccessfully with etanercept before canakinumab. HIDS
patients showed recurrent fever attacks together with
gastrointestinal symptoms and enlarged lymphadenopathies. They
were given colchicine before the diagnosis of HIDS. All three
TRAPS patients had recurrent fever attacks and were given
colchicine before canakinumab. One of the patients with TRAPS
also had IgA nephropathy and was given methylprednisolone and
cyclosporine before canakinumab [17]. The DADA2 patient had
hepatosplenomegaly, nephrotic range proteinuria, low serum
immunoglobulin G, and immunoglobulin M levels and was diagnosed
with renal amyloidosis. He was given methylprednisolone,
cyclosporine, and colchicine before canakinumab [2], colchicine
treatment was continued thereafter with canakinumab.
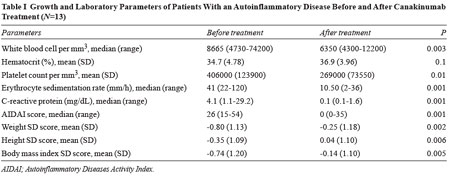
Disease activities of the patients
were evaluated, except for the DADA2 patient because of the
unavailability of activity score. Only one FMF patient with
chronic arthritis was not in remission according to the AIDAI
score after CAN. White blood cell and platelet counts, ESR, and
CRP levels significantly decreased after canakinumab (Table
I).
The mean weight, height, and BMI
SD scores after therapy were significantly higher than before (Table
I). The growth parameters after canakinumab did not differ
significantly with gender and age-group at diagnosis (<6 year
and
³6
year) or follow-up duration (less than or more than 3 years).
Discussion
In the present
study, mean height, weight, and BMI SD scores of the patients
with autoinflammatory diseases significantly increased after
canakinumab treatment. Growth parameters after canakinumab did
not differ according to gender, the duration of diagnostic delay
and age at diagnosis. Controlling disease activity with the drug
in these patients suppressed ongoing inflammation, which may
explain the significant improvements in growth parameters.
We recently reported the canakinumab experience in 14
colchicine-unresponsive FMF patients. Attack frequency,
proteinuria, and acute phase reactants, including ESR and CRP,
were significantly decreased after the drug [16]. In the present
study, depicting improvement in growth parameters, acute phase
reactants and disease activity in patients with AIDs on
canakinumab further suggests its effectiveness in those
patients.
The effect of anti-interleukin 1 blocking agents, either
anakinra or canakinumab, were also presented in eight
colchicine-unresponsive FMF patients in a previous report [18].
Moreover, the effectiveness of canakinumab for the treatment of
autoinflammatory diseases has been investigated in another
study, in where colchicine resistant FMF, MKD and TRAPS patients
were included. It
was efficacious in controlling and preventing flares in those
patients [5].
Even though, the heterogeneity of the study population, small
number of patients, retrospective design and data collection are
the limitations, the rarity of the autoinflammatory diseases and
having no data on growth parameters in those treated with
canakinumab make the present study valuable. Another limitation
of the study is the lack of investigation about environmental
factors, including diet and physical activity. Therefore,
prospective and even multicenter studies conducted on a large
number of AIDs patients are needed to clarify the effect of
canakinumab on growth in patients with auto- inflammatory
disease.
Contributors:
SB, MY: conceptualized and designed the study, drafted the
initial manuscript, and reviewed and revised the manuscript;
RMKE,DD: collected data, carried out the initial analyses, and
reviewed and revised the manuscript; DUA, DD: designed the data
collection instruments, and coordinated and supervised data
collection, and critically reviewed the manuscript. All authors
approved the final manuscript as submitted and agree to be
accountable for all aspects of the work.
Funding:
None; Competing interest: None stated.
What This Study Adds?
•
Canakinumab treatment has positive effects on growth
parameters in children with autoinflammatory diseases. |
|
References
1.
Oda H, Kastner DL. Genomics, Biology, and Human Illness:
Advances in the monogenic autoinflammatory diseases. Rheum Dis
Clin North Am. 2017;43:327-45.
2.
Kisla Ekinci RM, Balci S, Bisgin A, Hershfield M, Atmis
B, Dogruel D, et al. Renal Amyloidosis in Deficiency of
Adenosine Deaminase 2: Successful Experience with Canakinumab.
Pediatrics. 2018;142:e20180948..
3.
van der Burgh R, Ter Haar NM, Boes ML, Frenkel J.
Mevalonate kinase deficiency, a metabolic autoinflam-matory
disease. Clin Immunol. 2013;147:197-206.
4.
ter Haar NM, Oswald M, Jeyaratnam J, Anton J, Barron KS,
Brogan PA, et al. Recommendations for the management of
autoinflammatory diseases. Ann Rheum Dis. 2015; 74:1636-44.
5.
de Benedetti F, Gattorno M, Anton J, Ben-Chetrit E,
Frenkel J, Hoffman HM, et al. Canakinumab for the
treatment of autoinflammatory recurrent fever syndromes. N Engl
J Med. 2018;378:1908-19.
6.
Ozen S, Kone-Paut I, Gül A. Colchicine resistance and
intolerance in familial mediterranean fever: Definition, causes,
and alternative treatments. Semin Arthritis Rheum.
2017;47:115-20.
7.
Balci S, Ekinci RMK, Bayazit AK, Melek E, Dogruel
D, Altintas DU, et al. Juvenile systemic lupus
erythematosus: A single-center experience from southern Turkey.
Clin Rheumatol. 2019;38:1459-68.
8.
Kisla Ekinci RM, Balci S, Akay E, Dogruel D, Altintas DU,
Yilmaz M. Disease severity and genotype affect physical growth
in children with familial mediterranean fever. Arch Rheumatol.
2019;34:i-vi. [Epub ahead
of print]
9.
Gutierrez-Suarez R, Ruperto N, Gastaldi R, Pistorio A,
Felici E, Burgos-Vargas R, et al. A proposal for a
pediatric version of the systemic lupus international
collaborating clinics/american college of rheumatology damage
index based on the analysis of 1,015 patients with
juvenile-onset systemic lupus erythematosus. Arthritis Rheum.
2006;54: 2989-96.
10.
Zung A, Barash G, Zadik Z, Barash J. Familial
mediterranean fever and growth: Effect of disease severity and
colchicine treatment. J Pediatr Endocrinol Metab.
2006;19:155-60.
11.
Yoldas TC, Cakar N, Basaran O, Acar B, Uncu N, Caycý FS.
The effect of colchicine and disease severity on physical growth
in children with familial mediterranean fever. Clin Rheumatol.
2016;35:1603-07.
12.
Livneh A, Langevitz P, Zemer D, Zaks N, Kees S, Lidar T,
et al. Criteria for the diagnosis of familial
mediterranean fever. Arthritis Rheum. 1997;40:1879-85.
13.
Ozen S, Demirkaya E, Duzova A, Erdogan O, Erken E, Gul A,
et al. FMF50: A score for assessing outcome in familial
mediterranean fever. Ann Rheum Dis. 2014;73:897-901.
14.
Piram M, Koné-Paut I, Lachmann HJ, Frenkel J, Ozen S,
Kuemmerle-Deschner J, et al. Validation of the
auto-inflammatory diseases activity index (AIDAI) for hereditary
recurrent fever syndromes. Ann Rheum Dis. 2014;73: 2168-73.
15.
Neyzi O, Gunoz A, Furman A, Bundak R, Gökçay G,
Darendeliler F, et al. Weight, height, head circumference
and body mass index references for Turkish children. Cocuk
Sagligi ve Hastaliklari Derg. 2008;51:1-14.
[article in Turkish]
16.
Kisla Ekinci RM, Balci S, Dogruel D, Altintas DU, Yilmaz
M. Canakinumab in children with familial mediterranean fever: A
single-center, retrospective analysis. Paediatr Drugs.
2019;21:389-95.
17.
Balci S, Kisla Ekinci RM, Melek E, Atmýþ B, Bisgin A,
Yilmaz M. Phenotypic variability in two patients with tumor
necrosis factor receptor associated periodic fever syndrome
emphasizes a rare manifestation: Immuno-globulin a nephropathy.
Eur J Med Genet. 2019; Oct 3:103780. [Epub ahead of print]
18.
Basaran O, Uncu N, Celikel BA, Taktak A, Gur G, Cakar N.
Interleukin-1 targeting treatment in familial Mediterranean
fever: an experience of pediatric patients. Mod Rheumatol. 2015;
25: 621-4.