|
|
|
Indian Pediatr 2015;52: 617-618 |
 |
Morbidity Profile of Adolescents Admitted in a
General Pediatric Ward
|
|
A Chakraborty, S Basu and B Rath
Department of Pediatrics Lady Hardinge Medical College
and Kalawati Saran Children’s Hospital, New Delhi, India.
Email:
[email protected]
|
|
We studied the morbidity pattern of inpatient adolescents over a period
of 17 months. Of 32115 admissions in this period, 2742 were adolescents
(39.7% females). 93.9% were partially immunized, 37.3% were
malnourished, 2.8% were overweight and 56% were anemic. Dengue and
dengue-like illness (528) were the most common illness.
Keywords: Disease, Outcome, Teenagers, Young
people.
|
|
Adolescents make-up 18% of the world’s population [1]. Adolescence and
young adulthood coincide with major changes in health problems [2,3] and
emergence of risk behaviors [4]. Yet extensive review of literature has
revealed scarce data on the morbidity pattern of adolescent patients in
India. Thus we conducted this study of demographic and morbidity profile
of adolescents admitted in pediatric wards.
This prospective study was conducted in the inpatient
general Pediatrics ward of Kalawati Saran Children’s Hospital, Lady
Hardinge Medical College (LHMC) for a period of 17 months. All
adolescents (10-18yrs) admitted for at least 48 hours were included in
the study. Patients in ICU or shifted from the ICU, those with
intellectual disability, and those who left against medical advice were
excluded. A structured form was used containing demographic data like
age, sex, educational status of the patient and their parents, family
income, nutritional status, hemoglobin levels, immunisation status and
diagnosis at discharge to assess the morbidity profile. For assessing
anemia and nutritional status, respective age-matched WHO data were used
[5, 6]
Of the total 32115 admissions, 2742 were adolescents
(39.7% females). 68.8% were aged between 10 and 13 years (early
adolescence), and 28.6% between 14 and 16 years (mid adolescence). Among
females, 14.0% were uneducated, 38.8% received primary education and
47.2% received secondary education. Whereas among males, these rates
were 10.9% 45.8% and 43.3%, respectively. Immunization status showed
that only 6.0% of the patients were immunised for age, and 11.4% were
not imunised. 56.0% of the patients were anemic, 37.3% were thin whereas
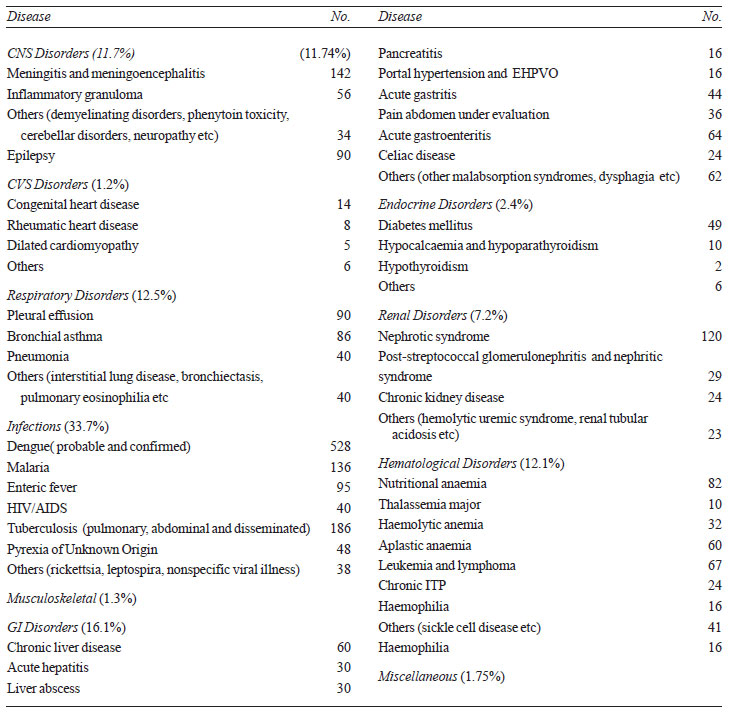
2.8% were overweight. System-wise distributions of the diseases (Table
I) shows the bulk of diseases as infectious. Dengue and dengue-like
illness were the commonest diagnosis.
|
TABLE I Disease Spectrum of Adolescents (N=2742)
|
 |
In this study, a higher proportion of male admissions
(60.2 %) were noted probably due to social reasons. 56% of the patients
were found to be anaemic which is considerably higher than previous
figure [7,8], probably a Berkesonian bias. 37.3% of the patients were
found to be undernourished, at par with most other studies [7,8].
Systemic infections was the commonest cause of admission (33.6%) in
contrast to Sachdeva, et al.[9], where the commonest cause of
admission was injury, poisonings, burns and accidents followed by
pregnancy (13.9%), but consistent with findings of Ojukwu, et al.
[10]. This difference is probably related to the sources of data (only
pediatrics ward in our study as compared to different wards in the study
by Sachdeva, et al. Overall hospital morbidity in this study,
like others from developing countries, is infectious in origin, which is
in sharp contrast to with the developed countries with non-infectious
causes including substance abuse, depression, obesity forming the bulk
[4]. Being a hospital-based data our findings cannot be extrapolated to
the general population, but in absence of any baseline data it can be
close approximation to the overall morbidity pattern.
Contributors: AC: Data acquisition, data
analysis, design of the study, revision of the manuscript for important
intellectual content and final approval; SB: Design of the study,
analysis, drafting and final approval of the manuscript; BR: analysis of
data, data acquisition, drafting of the manuscript and final approval.
Funding; None; Competing interests: None
stated.
References
1. WHO. Broadening the Horizon Balancing Protection
and Risk for Adolescents.; 2001:1. Available at:
http://whqlibdoc.who.int/hq/2001/WHO_FCH_CAH_01.20. pdf?ua=1.
Accessed September 12, 2014.
2. Kleinert S. Adolescent health: an opportunity not
to be missed. Lancet. 2007;369:1057-8.
3. Patton GC, Coffey C, Sawyer SM, Sawyer SM, Viner
RM, Haller DM, et al. Global patterns of mortality in young
people: a systematic analysis of population health data. Lancet.
2009;374:881-92.
4. Patton GC, Viner R. Pubertal transitions in
health. Lancet. 2007;369:1130-9.
5. WHO. Haemoglobin concentrations for the diagnosis
of anaemia and assessment of severity. Available at:
http://www.who.int/vmnis/indicators/haemoglobin.pdf. Accessed
September 12, 2014.
6. WHO. | BMI-for-age (5-19 years). Available at:
http://www.who.int/growthref/who2007_bmi_for_age/en/. Accessed
September 12, 2014.
7. Dambhare DG, Bharambe MS, Mehendale AM, Garg BS.
Nutritional status and morbidity among school going adolescents in
Wardha, a peri-urban area. Online J Heal Allied Sci. 2010;9:1-3.
Available at: http://cogprints.org/7002/1/2010-2-3.pdf. Accessed
September 12, 2014.
8. Basu S, Basu S, Hazarika R, Parmar V. Prevalence
of anemia among school going adolescents of Chandigarh. Indian Pediatr.
2005;42:593-7.
9. Sachdeva S, Kapilashrami MC, Sachdev TR.
Adolescent profile: hospital record based study. Int J Adolesc Med
Health. 2010;22:561-6.
10. Ojukwa J, Ogbu C. Morbidity pattern in
adolescents attending the ambulatory care unit in Abakliki. Niger J
Pediatr. 2007;32:33-9.
|
|
|
 |
|
