Traditional medical education is built around
educational learning objectives, using processes to ensure that a
graduate has knowledge, skills and attitude to perform competently [1].
Acquisition of knowledge, skills and attitudes is used as a surrogate
marker for competency; unfortunately, there is a disparity between the
intended outcome (competent medical practitioner) and the enacted
curriculum. The problem is universal – educators globally report that
training which concentrates on the acquisition of knowledge and skills
may not result in a competent practitioner; learners may not be able to
perform satisfactorily, or with confidence, in real time [2,3]. There is
a need, therefore, to turn the focus of training programs towards the
acquisition of competencies [4].
Assessment of Competencies
The concept of competency-based medical education
(CBME) has been dealt with earlier [5]. To recapitulate, competency is
the measure of a person’s expertise to perform the tasks he has been
trained to perform. A competency-based curriculum is designed backwards,
beginning from the outcome, i.e. by first defining the expected
roles of a medical practitioner (competency domains) in the context of
local health needs, and then designing the curriculum around those
outcomes (outcome-based curriculum) [1,6]. Box 1 lists the
various nuances of the word ‘competency’ in reference to CBME.
|
Box 1: Definitions Related to Competency
|
|
Competency
The ability that must be acquired in
order to be called competent (the medical practitioner acquires
knowledge, skills and attitude and is observed to be able to
perform – the Student/Practitioner has competency in managing a
child with diarrhea).
Competent
The person has the competency (in a
certain context at a certain stage of medical education or
practice – the Student/Practitioner is competent to counsel
parents of children with diarrhea presenting to a pediatric
OPD).
Competence
The performance (the student /
practitioner consistently performs expertly, adapting to
different contexts and degrees of complexity – the
Student/Practitioner manages, with competence, any child with
diarrhea).
Put simply; Competency: Thing to be able to
do expertly; Competent: Can do it; Competence: Does it
|
Competencies are the building blocks of CBME.
Assessment systems must be able to capture the actual competencies
acquired, unlike in the traditional, process-based program where
competence is presumed once the learner acquires knowledge and skills.
Designing assessment for CBME is challenging. Educators worry that
competency-based curricula may assure acquisition of individual
competencies, but an integration across different competency domains may
not result [7]. For example, a student may acquire expertise in medical
knowledge and be a competent communicator, but may not be able to apply
both in an integrated manner during actual patient care. Another
anticipated problem is that a learner who is competent in one setting or
context (stable patient/ward) may not be as competent in another setting
(hemodynamically unstable patient/emergency) [6]. Finally, CBME focuses
on abilities, which means a learner shows how able he is; there may be a
disparity in how able he is and how he actually performs in varying,
real-life, clinical situations [2]. Clearly then, an assessment system
that measures competency in an integrated manner, across a variety of
clinical situations, and during actual performance would be ideal for
CBME [6,7]. Entrustable Professional Activities (EPA) were developed to
address these gaps between competency and actual practice.
Terminology:Trust, Competence and Milestones
Trust
As a routine, students start with simple, easy to
perform tasks, and move along over time, to more complex
responsibilities. Supervision, mandatory at first, becomes less
essential as competence improves. Finally, once the teacher begins to
trust that the trainee has the ability and the will to apply competence,
supervision becomes unnecessary. Trust, thus, is generated by real-time
experiences when the trainee performs tasks at an acceptable level of
competence [4]. Essentially, degree of trust (entrustability) is
inversely proportional to degree of supervision – as trainee competence
improves, trust builds, and the need for supervision reduces.
Decisions to trust are made on day-to-day basis
(ad-hoc entrustment), but must also be made at the end of a term/course
(summative entrustment) [6]. Thereafter, the learner is permitted to
enact the EPA without supervision. Besides trainee competence, other
factors that facilitate trust include trainee integrity,
conscientiousness, reliability, and self-reflection i.e. a
trainee who is aware of his own limitations and asks for help [9,10]. A
teacher may trust a learner without even observing him, based on prior
credentials (presumptive trust), or may form a good impression at the
first encounter (initial trust); however, grounded trust can only occur
over a period of repeated interactions and observations. Entrustment
decisions (whether or not to trust the learner to perform the task)
should be based on grounded trust [4].
Competence
From the perspective of Miller’s pyramid model of
clinical competence, a competent person ‘shows how’ [11]. In EPA, the
key word is trust – do you trust this learner to take
responsibility, without supervision, for this particular professional
task? If the answer is yes, the learner has demonstrated competence in
the performance of the task. Entrustability is achieved when a learner
performs a professional activity with such mastery that he can be
trusted to perform it unsupervised in future. From the perspective of
Miller’s pyramid, he ‘does’. EPAs, thus, are professional tasks that
bridge the gap between being competent and actually demonstrating it in
practice [6].
To perform a single EPA, the learner may require to
be competent in several areas. For example, when we consider the EPA of
‘eliciting a basic medical history’, the student would have to be
proficient in the competencies of ‘medical knowledge’, ‘patient care’
and ‘interpersonal and communication skills’. Likewise, to ‘show’ a
single competency, the learner may have to demonstrate proficiency in
several EPAs. For example, to show competency in ‘interpersonal and
communication skills’, the learner should be able to elicit a basic
history, counsel patient about dietary practices, take informed consent
for procedures/surgery, and counsel relatives about a terminally ill
patient. Box 2 summarizes the difference between learning
objective and EPA.
|
Box 2: Learning Objective Versus
Entrustable Professional Activity
|
|
Learning objective
• What learners are expected to be able to do
at the end of an instructional intervention; the
desired
outcome of the intervention.
• It is the minimum demonstrable and
assessable
change in knowledge, skill or attitude after which
the learner
is deemed to have successfully
completed
the course. Competence is assumed.
Entrustable professional activity
• The
professional task that a learner is entrusted to perform without
supervision at any time during the training, or at the end of
it.
• The prerequisite to trusting a learner to
perform a task
unsupervised
is his becoming competent at it. Thus,
EPA is not
merely acquisition of knowledge, skills and
attitude,
but an assessment of acquisition of one or more interlinked
competencies.
|
Milestones
Competence – and therefore trust – builds over a
period of time. When we consider the competency of ‘interpersonal and
communication skills’, some aspects (sub-competencies) can be expected
to be expertly demonstrated earlier in the learning curve while others
would require more time. When all the particular sub-competencies –
necessary to be shown before we can say that a particular competency has
been achieved – are arranged on a time line, we get what are known as
milestones. Each milestone signifies steps in the learner’s progression;
at each subsequent step, the task that the learner is expected to
perform competently, without supervision, gets more and more complex
[2,8,12-14]. For example, a student should become competent in eliciting
a basic medical history from a patient or his relatives within a month
of his posting in that discipline; however, his ability to expertly
counsel a patient to give consent for a procedure/surgery may be
expected to reach expert level only at the end of final year or in
internship. Clearly, competencies, EPA’s and milestones are inextricably
linked to each other (Fig. 1 and 2).
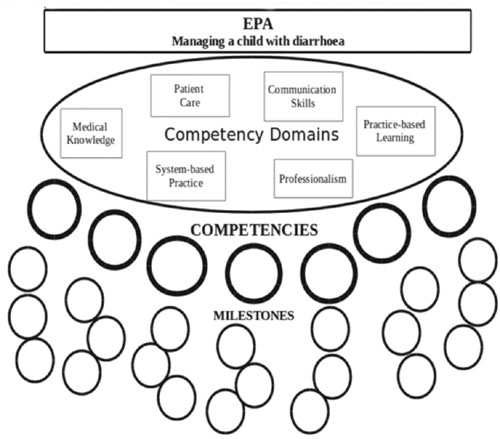 |
|
Fig. 1 Correlation between EPA,
competencies and milestones.
|
Designing Entrustable Professional Activities
There are many tasks expected of a medical student in
each discipline; how then do we set about deciding which to include in
the list of EPAs? As a guideline, you should ask yourself what tasks a
trainee can be scheduled to perform and whether an entrustment decision
for unsupervised practice of that task can be documented.
When it is a question of ad hoc entrustment, there
will be many tasks that one can enlist, like ‘able to assess vital
signs’, or ‘able to measure intraocular pressure’; however, EPAs that
lead to grounded trust – summative entrustment decisions, after
which we trust/permit the student to perform that task unsupervised –
should assess broad responsibilities and should be limited in number.
Step 1: Identify Attributes of EPA
Every specialty should identify activities that are
core or critical, and are expected to be entrusted to a sufficiently
competent trainee [1,15]. Include only those activities that a
professional must master in order to practice with competence. An
activity must fulfill the following criteria to make it an effective
measure of competence [2,14,15]:
1. An EPA should be suitable for entrustment,
in that it should be
(a) executable independently (without
supervision) by an individual learner within a definite
time-frame;
(b) it should be observable (by an
expert); and
(c) both the process and the outcome
should be measurable.
For example, ‘inserting an IV-line’ –can be executed
by an individual independently, within a time-frame; it is observable,
and both the process and the outcome (fluid flows freely into the vein)
are measurable – this is an EPA.
2. It should be an essential professional
activity in the specialty, preferably a real-life patient-care
episode that requires specialized knowledge, attitude and skills
such that only trained, qualified persons will perform them. For
example, ‘performing a lumbar puncture’ is a specialized skill
learned through training, while ‘measuring urine output’ does not
require specialized knowledge or skill – even a nursing orderly can
perform it. The latter, therefore, is not suitable to be translated
into an EPA.
3. It should reflect relevant competencies – the
EPA should lead directly to one or more of the competencies that are
required to be attained at the end of the program.
Step 2: List Areas of Competence in Different Domains
All the activities for a particular specialty should
be listed, and each described briefly in a statement that tells what is
expected of the learner. Against each EPA, one or more of the
competencies that can be assessed should be recorded. For example,
performing neonatal resuscitation requires competence in medical
knowledge, patient care, procedural skills, and interpersonal and
communication skills. A trainee would have to possess knowledge and
skills to perform the procedure, would have to communicate with the
child’s care-givers on the need for and the risks of the procedure, and
work in a team with a nurse or a technician.
Step 3: Create Milestones
Milestones are the observable and measurable steps
taken by the trainee as he moves from newbie to expert [3,14,16];
experienced specialists instinctively know these steps for their
specialty. Milestones encourage trainees to progress towards appropriate
levels of competence. Simpler, more frequently done, or essential tasks
should be mastered sooner. The milestones chosen should be tailored to
the program; they should be based on the local resources, and on the
knowledge, skills, and attitudes required to meet the outcomes expected
of the particular health care system. Milestones may be stratified as
shown in Fig. 2.
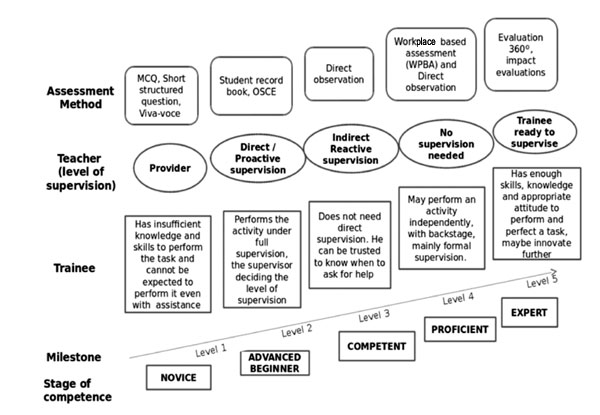 |
|
Fig. 2 Milestones: steps in the
learner’s progress. Milestones define the abilities expected of
the learners as they progress through training. They integrate
the cognitive, psychomotor and behavioral domains. Milestones
are observable and set the stage for assessment of the
entrustable professional activities.
|
Milestones should be detailed keeping in mind each of
the five levels so that both the trainee and the supervisor have a
benchmark against which to assess the trainees performance. Each level
should have a description of observable behavior appropriate for that
level, with the behavior getting more and more expert as one advances up
to level five; level five should detail the behavior expected from a
master practitioner.
Step 4:
Align the Milestone to Assessment (Table I)
Figure out what methods will help the teacher in
deciding on whether to entrust a trainee with a task under no or minimal
supervision [6]. The method must assess skills and attitude mainly, but
some degree of assessment of knowledge may be required [2]. Methods
could include direct observation, multisource feedback, and chart audit;
teachers may use existing methods or devise new ones. The assessment may
involve more than one teacher and should be a formal process. Teachers
should be trained in the formulation and assessment of EPAs.
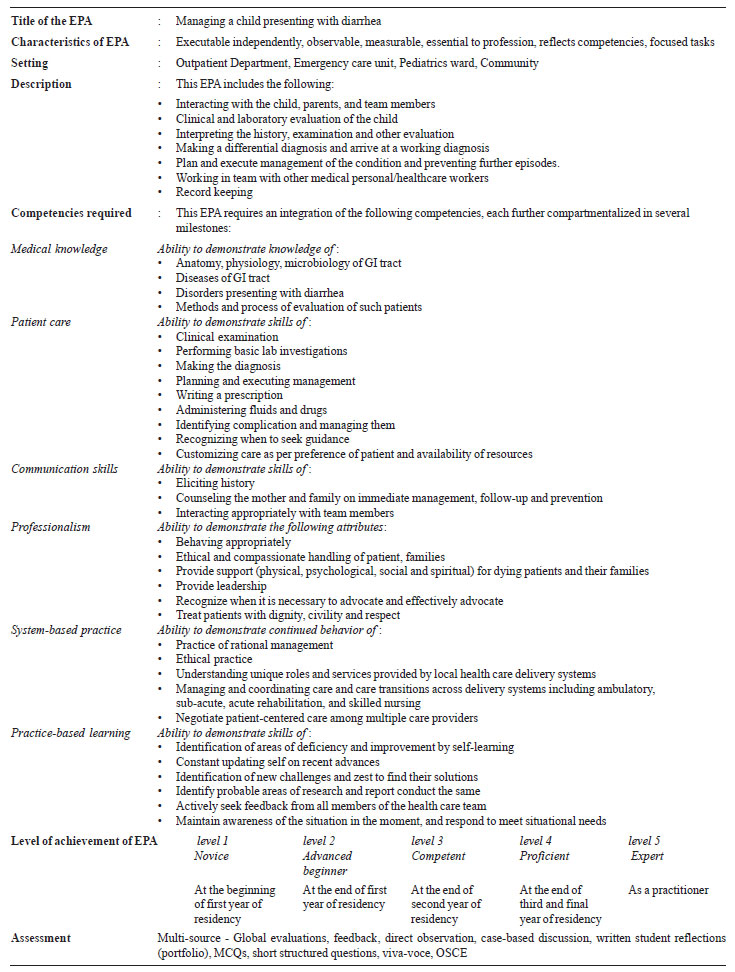
Formulating an EPA [5]
To be unambiguous and effective, each EPA must
include a short title, the target student, and setting(s) where it may
be performed/assessed. The activity should be described in detail
mentioning what it is limited to; the relevant competencies should be
listed, including what knowledge, skills and attitudes are required to
achieve competency; and milestones should be detailed. Finally, give the
assessment method i.e. how the teacher(s) will determine whether the
learner can be trusted to competently perform the activity without
supervision. An example, with essential components emboldened is
provided in Table I.
|
TABLE I Example of an Entrustable
Professional Activity for Training and Evaluation of a Resident
in Pediatrics
|
 |
Awarding an EPA to the Learner [4]
Based on performance in the EPA, each student finds a
place on the entrustment scale (entrustment is inversely proportional to
degree of supervision) as follows:
Level 1. Not ready to be entrusted with the task
(no permission to enact the EPA; observes the activity).
Level 2. Ready to perform EPA under direct,
pro-active supervision (supervisor present in the room).
Level 3. Ready to perform EPA under indirect,
reactive supervision (supervisor available within minutes).
Level 4. Ready for unsupervised practice (distant
oversight).
Level 5. Ready to supervise junior learners in
the performance of the EPA
If the learner has demonstrated over time,
repeatedly, that he is capable of performing the task competently, then
the supervisor knows that the learner is ready to perform without
supervision, and the EPA can be awarded to that learner. Thereafter, the
learner is allowed to perform that task without supervision. The
particular specialty may decide when to award the EPA to the trainee.
For some activities, it may be awarded when the trainee reaches level-4
of competence, but for others, particularly simple, commonplace or
essential activities, level-5 may be desirable. At the end of the
assessment (formative), the teacher can decide which EPA can be
entrusted to the trainee, and which he is as yet not ready to be trusted
with. As the learner progresses towards competency, he/she should be
able to achieve EPAs of increasing difficulty, risk, or sophistication.
A trainee trusted to carry out critical EPAs could be considered as
performing well. A trainee who has not achieved level 4 or level 5 in
one or more critical competencies may be required to continue in the
course beyond its usual, expected duration. When an EPA is awarded, the
learner is given a STAR (Statement of Awarded Responsibility) [6].
Advantages of EPA [4,6,17]
• It measures real time performance, which is
better than assuming that the trainee will be able to perform.
• It utilizes an expert supervisor’s subjective,
day-to-day observations of the trainee against a competency
benchmark.
• It improves patient safety by ensuring that a
trainee asked to perform a task without supervision has previously
demonstrated a high level of competence in that task.
• It encourages curriculum planners to focus on
the outcomes of training as well as the process.
• It allows trainees to evaluate their learning
against expectations listed in the EPA and milestone document.
• Medical competence gets measured by a portfolio
of EPAs. The process is dynamic and the list may be expanded over a
lifetime, with new EPAs being added, or older ones being re-learned,
when required.
• Trainers, on a daily basis, have to take the
call on whether or not to delegate professional activities to
learners. Trust must be earned by demonstrating definite skills
during activities when the supervisor is present. A trainee who is
eventually entrusted to carry out all the critical EPAs could be
said to be competent in the specialty. As suggested by Ten Cate, in
order to promote the acquisition of competencies, perhaps medical
training could change from fixed-length, variable-outcome programs
to fixed-outcome, variable-length programs [1].
Role of the Medical Council of India (MCI) and the
Indian Academy of Pediatrics (IAP)
The Vision-2015 document promulgated by the MCI
emphasizes a competency-based curriculum [18]. Five competency domains
(roles) are outlined: Clinician, who understands and provides
preventive, promotive, curative, palliative and holistic care with
compassion; Leader and member of the health care team and system;
Communicator with patients, families, colleagues and community; Lifelong
learner committed to continuous improvement of skills and knowledge;
and, Professional who is committed to excellence, is ethical, responsive
and accountable to patients, community, and profession. They have
recommended the building of competency based modules. The IAP - and in
fact all disciplines - should take it up from there [19]. The first step
is capacity building i.e. training faculty in the principles of CBME and
EPA. This can be followed by formulation of EPAs for both undergraduate
and post-graduate studies.
References
1. Ten Cate O. Entrustability of professional
activities and competency-based training. Med Educ. 2005;39:1176-7.
2. Englander R, Carraccio C. From theory to
practice: making entrustable professional activities come to life in
the context of milestones. Acad Med. 2014;89:1321-3.
3. Ten Cate O. Competency-based education,
entrustable professional activities, and the power of language. J
Grad Med Educ. 2013;5:6-7.
4. Ten Cate O. Trust, competence, and the
supervisor’s role in postgraduate training. BMJ. 2006;333:748-51.
5. Modi JN, Gupta P, Singh T. Competency-Based
Medical Education. Indian Pediatr. 2015; 52:413-20.
6. Ten Cate O. Nuts and bolts of entrustable
professional activities. J Grad Med Educ. 2013;5;157-8.
7. Chen HC, van den Broek WES, Ten Cate O. The
case for use of entrustable professional activities in undergraduate
medical education. Acad Med. 2015;90:431-6.
8. Martinez J, Phillips E, Harris C. Where do we
go from here? Moving from systems-based practice process measures to
true competency via developmental milestones. Med Educ Online.
2014;19:24441.
9. Wijnen-Meijer M, van der Schaaf M, Nillesen K,
Harendza S, Ten Cate O. Essential facets of competence that enable
trust in medical graduates: a ranking study among physician
educators in two countries. Perspect Med Educ. 2013;2:290-7.
10. Hauer KE, Ten Cate O, Boscardin C, Irby DM,
Iobst W, O’Sullivan PS. Understanding trust as an essential element
of trainee supervision and learning in the workplace. Adv Health Sci
Educ Theory Pract. 2014;19:435-56.
11. Miller GE. The assessment of clinical
skills/competence/performance. Acad Med. 1990;65(9 Suppl):S63-7.
12. Green ML, Aagaard EM, Caverzagie KJ, Chick
DA, Holmboe E, Kane G, et al. Charting the road to
competence: developmental milestones for internal medicine residency
training. J Grad Med Educ. 2009;1:5-20.
13. Carraccio C, Benson B, Burke A, Englander R,
Guralnick S, Hicks P, et al. Pediatrics milestones. J Grad
Med Educ. 2013;5:59-73.
14. Hicks PJ, Englander R, Schumacher DJ, Burke
A, Benson BJ, Guralnick S, et al. Pediatrics milestone
project: next steps toward meaningful outcomes assessment. J Grad
Med Educ. 2010 2:577–84.
15. Hauer KE, Kohlwes J, Cornett P, Hollander H,
Cate O ten, Ranji SR, et al. Identifying Entrustable
Professional Activities in Internal Medicine Training. The
Accreditation Council for Graduate Medical Education Suite 2000, 515
North State Street, Chicago, IL 60654; 2013 Mar 28. Available from:
http://www.jgme.org/doi/full/10.4300/JGME-D-12-00060.1.
Accessed March 29, 2015.
16. Sklar DP. Competencies, milestones, and
entrustable professional activities: what they are, what they could
be. Acad Med. 2015;90:395-7.
17. Ten Cate O, Scheele F. Competency-based
postgraduate training: can we bridge the gap between theory and
clinical practice? Acad Med. 2007;82:542-7.
18. Vision 2015. Medical Council of India.
Available from: http://www.mciindia.org/tools/announcement/MCI_booklet.pdf.
Accessed March 29, 2015.
19. Swing SR, Beeson MS, Carraccio C, Coburn M, Iobst W, Selden NR,
et al. Educational milestone development in the first 7
specialties to enter the next accreditation system. J Grad Med Educ.
2013;5:98-106.


