|
|
|
Indian Pediatr 2013;50: 709-710 |
 |
Delayed Presentation of Traumatic
Diaphragmatic Hernia
|
|
K Jagadish Kumar and *MG Anil Kumar,
Department of Pediatrics and *Pediatric Surgery, JSS
Medical College, JSS University, Mysore, India.
Email: [email protected]
|
A 10-year-old boy presented with abdominal pain around the
umbilicus since 8 hours, 4 episodes of non-bilious vomiting
and pain in the left shoulder since 5 hours. There was no
history of fever or bowel disturbances. On examination his
general condition was stable. Per abdomen examination
revealed tenderness around the umbilicus. Examination of
other systems was unremarkable. He had history of chest
trauma 7 months back. At that time examination revealed
wound measuring 4×2 cm below and lateral to left nipple with
normal vitals. Respiratory and abdominal examination was
unremarkable. Chest X-ray, sonography and CT scan
were normal. Debridement and suture of the wound was done
and child discharged after 5 days.During the second
admission, his blood counts, urine examination, serum
amylase, kidney function test and liver enzymes were within
normal limits. Chest X-ray revealed non-visualization
of left diaphragm and presence of distended bowel loops. CT
scan showed disrupted left hemidiaphragm with herniation of
bowel loops (Fig.1). On laparoscopy, left
diaphragm opening was noticed with colon and omentum as
contents. Surgeon tried to pull the contents back to abdomen
but could not. Therefore laparotomy was performed, contents
were reduced (colon was healthy) and closure of diaphram
opening was done. Child was discharged after 5 days.
 |
|
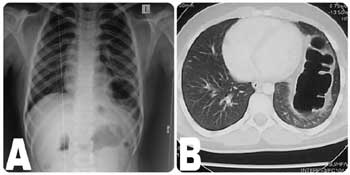
Fig. 1 (a) The chest X-ray
shows non-visualization of left diaphragm and
presence of distended bowel loops; (b) Axial post-IV
contrast CT through the lower chest showing
herniated bowel loops in the left lung field.
|
Traumatic diaphragmatic hernia due to
blunt trauma is rare in children and initial diagnosis is
usually difficult because the early clinical and
radiological findings are not clear [1,2]. Delayed
presentation of rupture of the diaphram is well recognized
in adults but exceptionally rare in children [1]. Grimes [3]
described the three phases of the rupture of the diaphragm.
The first acute phase is at the time of the injury to the
diaphragm, the second delayed phase is because of transient
herniation of the viscera accounting for absence or
intermittent non specific symptoms and the third obstruction
phase due to complication of a long standing herniation,
maninifesting as obstruction and strangulation [3]. Despite
techno-logical advances, 30-50% of traumatic diaphragmatic
ruptures are missed on initial presentation, as in our case
[4]. Only 25% to 50% of cases will be detected by initial
chest radiograph, with an additional 25% with subsequent
films [5]. Chest X-ray findings include distortion of
diaphragmatic margin, elevated hemidiaphragm (>4 cm higher
on left vs. right) and bowel loops in the lung space
[4, 5]. Conventional CT scan has been reported to have a
sensitivity of 14%-82% with a specificity of 87%
[5].Consistent CT findings include the "collar sign" which
is a focal constriction of abdominal viscera (most common),
intrathoracic herniation of abdominal contents, and
discontinuity in the diaphragm [4]. During the first
admission of this child with trauma, both chest X-ray
and CT scan were normal. On the second admission, he had
typical gastrointestinal symptoms with left shoulder pain
and X-ray showed classical picture of diaphragmatic
hernia which was confirmed on CT. To conclude, even though
diaphragmatic hernia is uncommon, high index of suspicion
should be kept in mind whenever there is a history of
trauma. Prompt diagnosis and treatment prevents
complications such as gangrene and perforation of herniated
organs.
References
1. Ninan G, Puri P. Late presentation of
traumatic rupture of the diaphragm in a child. BMJ.
1993;306:643-4.
2. Okan I, Bas G, Ziyade S, Alimoglu O,
Eryilmaz R, Guzey D, et al. Delayed presentation of
posttraumatic diaphragmatic hernia. Ulus Travma Acil Cerrahi
Derg. 2011;17:435-9.
3. Grimes OF. Traumatic injuries of the
diaphragm. Diaphragmatic hernia. Am J Surg. 1974;128:175-81.
4. Walchalk LR, Stanfield SC. Delayed
presentation of traumatic diaphragmatic rupture. J Emerg
Medi. 2010;39:21-4.
5. Lal S, Kailasia Y, Chouhan S, Gaharwar APS,
Shrivastava GP. Delayed presentation of post traumatic
diaphragmatic hernia. J Surg Case Rep.
2011;7:6.
|
|
|
 |
|
