|
|
Research Paper Indian Pediatrics 2008; 45:559-563 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Outcome in West Syndrome |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Natwar Lal Sharma and Venkataraman Viswanathan From the Department of Pediatric Neurology, Kanchi Kamakoti CHILDS Trust Hospital, Chennai, India. Correspondence to: Dr Natwar Lal Sharma, G-3, Mansarovar Apartments, No. 9, 5th Street, Thirumurthy Nagar, Nungambakkam, Chennai 600 034, India. E-mail: drnutties2000@yahoo.co.in Manuscript received: February 12, 2007; Initial review
completed: March 20, 2007;
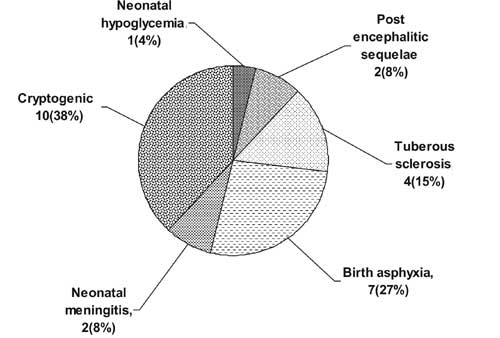
Introduction West syndrome consists of a characteristic triad of infantile spasms, arrest of psychomotor develop-ment, and hypsrarrhythmia; although diagnosis can be made even if one of the three elements is missing(1). The prognosis of West syndrome is poor despite treatment(2-6). Overall 5-12% of patients have normal mental and motor development. Approximately one-half are left with motor impairment and 70-78% are mentally retarded. The prognosis is better in the idiopathic or cryptogenic cases without known etiologic factor, and those having normal development status before the onset of the spasm, and normal neuroimaging prior to therapy. Among this group of infants, 37 to 44% are neurologically and cognitively normal at long-term follow-up. Earlier studies(3,4) observed that in the subgroup of cryptogenic patients, a delay in initiation of treatment may be associated with worse outcome. In three series(4,6,7) with larger number of patients and longer follow up time, a short time between onset and treatment correlated with a more favorable outcome than a long lag in institution of ACTH. A study(8) concluded that treatment lag is possibly a prognostic factor. Methods This was a prospective study carried out in the Department of Pediatric Neurology, Kanchi Kamakoti CHILDS Trust Hospital, between January 2003 and August 2004 after seeking ethical clearance from the Institutional Ethics Committee. All children with the classical triad of infantile spasms, psychomotor retardation and EEG pattern of hypsarrhythmia or modified hypsarrhythmia were included. Children who had received ACTH (adrenocorticotrophic hormone) injection previously were excluded. Informed consent was obtained from each child’s parent or guardian after explaining the protocol. Details of history and physical examination were recorded. Baseline developmental status was assessed by CMC scale(9). All children were subjected to complete blood count, liver function test, urine screening for inborn errors of metabolism, and EEG. Neuro-imaging was done wherever feasible. All children were started on ACTH and sodium valproate (20-40 mg/kg/day). ACTH was of synthetic origin (porcine sequence) as carboxy-methylcellulose complex in water. ACTH was given at a dose of 3 IU/kg everyday IM for the first week, followed by every alternate day for 2 weeks and then twice a week for 4 weeks, a total period of about 7 weeks and then discontinued(6). Other drugs including clonazepam, clobazam, lamotrigine, and vigabatrin were added as needed for seizure control. Response to treatment was assessed based on improvement on EEG, seizure count and develop-mental assessment. All children were followed up for 12-18 months (once a week for 1 month, once a month for 3 months and once in 2 months thereafter). During follow-up, children were assessed for change in seizure status, developmental assessment based on CMC scale which included 11 parameters - attachment behavior, visual attention, auditory attention, communication, behavior, motor attention, motor functions, hand functions, play behavior, sleep pattern and feeding with individual scores for each of them. Adverse effects of the drugs were also noted. Follow up EEG was done at the end of ACTH therapy (around 2 months) and one year from the onset of treatment. Significance of difference in continuous variables like development score, seizure control, different time lag and drugs was determined using the Mann-Whitney U test. Categorical variables like seizure control, EEG at follow up, response and relapse, were assessed by Chi-square test. Significance was determined at the 5% level, except for the different domains of the CMC scale, in which significance was determined at 0.05% level, in order to account for the multiple comparisons. Statistical analysis was performed using SPSS for Windows version 11.0. Results Thirty two children were initially enrolled; 4 discontinued the treatment and 2 were lost to follow up. Of the remaining 26 children, there were 14 boys and 12 girls. The average age of onset was 7±3 months (range 2-18 months) and mean age of presentation was 12.2±8.9 months. Twenty-four children (93.4%) presented within first year of life; most 19 (73.1%) had flexor spasms, 6 (23.1%) had mixed spasms and only 1 (3.8%) had extensor spasm. Etiology of West syndrome was identified in 16 (61.5%) children (symptomatic) and 10 (38.5%) remained cryptogenic. The etiology of infantile spasms is depicted in Fig. 1. Neuroimaging (CT/MRI brain) was available for 24 children (14 normal, 4 cerebral atrophy, 4 multiple tubers, 1 periventricular leucomalacia and 1 parieto-occipital infarct).
Mean cessation time of seizures (mean±S.D) was 2±2 weeks. Twenty two (84.6%) children responded, of whom 7(31.8%) relapsed; 4 (15.2%) children did not respond. EEG at follow up at the end of 1 year was normal in 11 (42.3%) and abnormal in 15 children (57.7%). The treatment lag was classified as <1 month (n=11; symptomatic-7, cryptogenic-4), 1-6 months (n=8; symptomatic-4, cryptogenic-4) and >6 months (n=7; symptomatic-5, cryptogenic-2). Anticonvulsants other than ACTH and sodium valproate were required in 18 (69.2%) children for seizure control. TABLE I Association of Time Lag with Developmental Score, Cessation Time, Seizure Control, Drugs, Response to Therapy, Relapse and Abnormal EEG at Follow-up
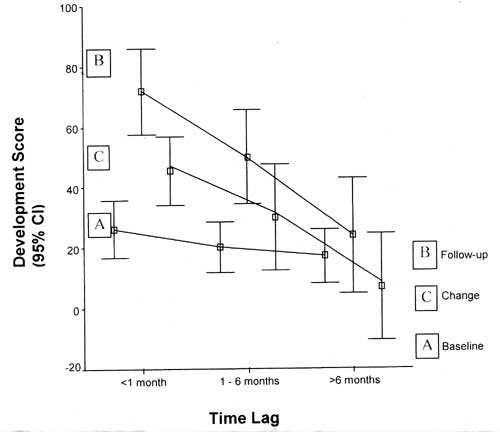
*Mann-Whitney U test; +Chi-square test; **Mann-Whitney U test with a=0.005, # Percentage reduction of seizure frequency from baseline. Table I compares seizure control, developmental progression with respect to each domain, response, relapse, number of drugs and EEG characteristics with time for treatment lag. Fig. 2 demonstrates that children with treatment lag of <1 month fared better in developmental score, as compared to the rest, at final follow-up. Association of seizure control (percentage reduction of seizure frequency from baseline) with change in development score is depicted in Table II. Children who had better seizure control fared better in development.
Adverse events noted with ACTH during the study were–sepsis in 1 (3.4%), hypokalemia in 3 (11.4%) and 4 had weight gain above the 95th centile which returned to baseline during follow up after stopping medication. There was no mortality during the study period. TABLE II Comparison between the Magnitude of Seizure Control with Change in Development Score
† Chi-square test, P = 0.041 Discussion Children with West syndrome who presented within 1 month from the onset of seizures had better seizure control. Also, children who presented early and had complete seizure control showed good improvement in development. Similar findings were reported in 4 large series(2,4,6,7). EEG findings and response rate was also comparable to previous studies(11,12). In one study of 37 patients(13) normal cognitive outcome was demonstrated in 100% children with cryptogenic spasms when treatment lag was <1 month. Our results on relation of seizure control and developmental progression were also similar to previous studies(4,6,14). Microcephaly did not affect the seizure outcome, which was also observed in another study(15). This study emphasizes the importance of diagnosing infantile spasms early and starting appropriate treatment. Even though some would consider one month as a long time before starting appropriate treatment for infantile spasms, these children appeared to do better than others both in terms of seizure control and developmental outcome. Interestingly in our case series, there was no significant difference in the outcome between the cryptogenic and the symptomatic group although the sample size is small and long term follow-up with detailed neuropsychological assessments is needed before one can come to definite conclusions. Acknowledgments The authors thank the Director of Kanchi Kamakoti Childs Trust Hospital for allowing us to do the study there, Dr Shrishu R Kamath for his special help and Dr M C Mathews, Developmental Pediatrics Unit, CMC, Vellore for permitting us to use the scale that his department has devised. Contributors: Both authors were involved in designing the study and preparation of the manuscript. VV will act as guarantor of the study. NLS was also involved in data collection, manuscript writing and analysis of data. Funding: None. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()