|
|
Case Reports Indian Pediatrics 2007;44:541-543 |
||||
|
Acute T-lymphoid and Megakaryoblastic Bi-lineal Leukemia in a Child |
||||
|
Upendra Srinivas From the Departments of Hematology and Medical Oncology,Dr. B.R.A. Institute Rotary Cancer Hospital, All India Institute of Medical Sciences, New Delhi 110 029, India. Correspondence to: Dr. Sameer Bakhshi,
Associate Professor of Pediatric Oncology, Department of Medical
Oncology, Dr. B.R.A. Institute Rotary Cancer Hospital, All India
Institute of Medical Sciences,
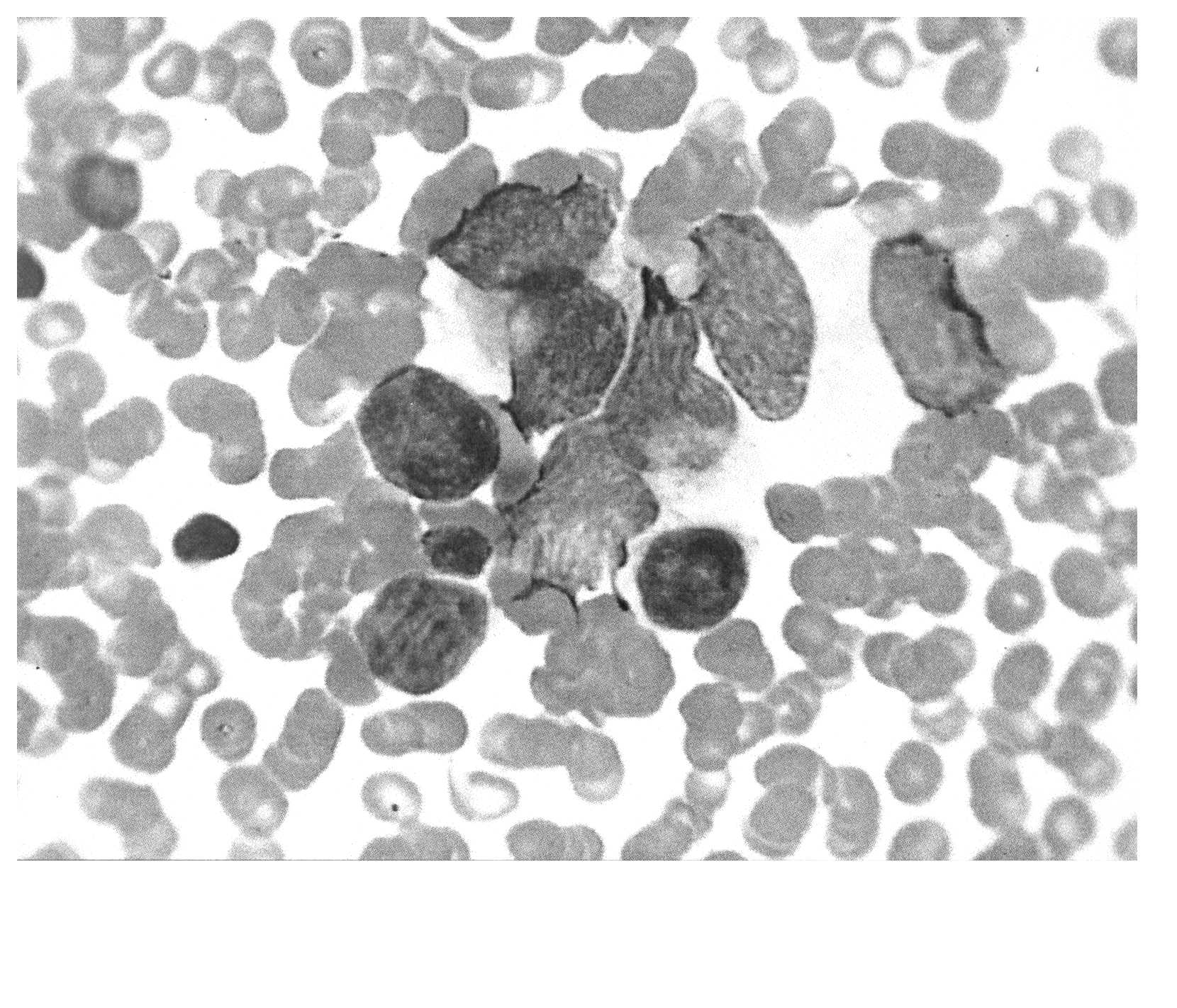
Case Report A 1½-year-old boy presented with complaints of high grade fever, petechial rash and abdominal distention of two weeks duration. There was no past history of bleeding manifestations. He was the first child of a non-consanguinous marriage, and his immunization status was appropriate for age. On examination he had severe pallor, petechiae over abdomen and upper limbs, hepatosplenomegaly of 2 cm each below costal margin. There was no significant lymphadenopathy and rest of the systemic examination was normal. Biochemical investigations revealed normal liver and renal function tests. Serological investigations for hepatitis B, hepatitis C and human immunodeficiency virus were negative. Chest radiograph was normal and ultrasound abdomen showed hepatosplenomegaly. Hemoglobin was 54 g/L; total leukocyte count was 29 × 109/L and platelet count 37 × 109/L. Peri-pheral smear examination showed 36% immature cells. Bone marrow smears showed 86% blasts composed of a mixture of two morphologically distinct cells (small and large blasts). The smaller blasts comprised 60% of immature cells; they were 1½-2 times the size of mature lymphocyte and had high nuclear/cytoplasmic ratio with scant rim of agranular cytoplasm, and coarse condensed chromatin; few of them showed prominence of nucleoli (Fig.1). The larger blasts composed 40% of the immature cells; they were 2½ to 3 times the size of mature lymphocyte with moderate to abundant amount of finely granular cytoplasm and coarse opened up chromatin with fairly conspicuous nucleoli in few of these cells (Fig.1). Cytochemical stains revealed positivity with Periodic-acid Schiff in smaller blasts and negativity with myeloper- oxidase (MPO), Sudan black, non-specific esterase and acid phosphatase. With a provisional morpho-logical diagnosis of acute bilineal leukemia an immunophenotyping by alkaline phosphatase-anti alkaline phosphatase (APAAP) was performed with anti-MPO, CDI3, CD33, CD2, CD7, CDI9, CD20 and CD 41. The smaller blasts showed CD2 positivity and the larger blasts showed CD41 positivity. Bone marrow cytogenetics was normal. A diagnosis of acute bilineal leukemia (T-lymphoid and megakaryocytic lineages) therefore was considered.
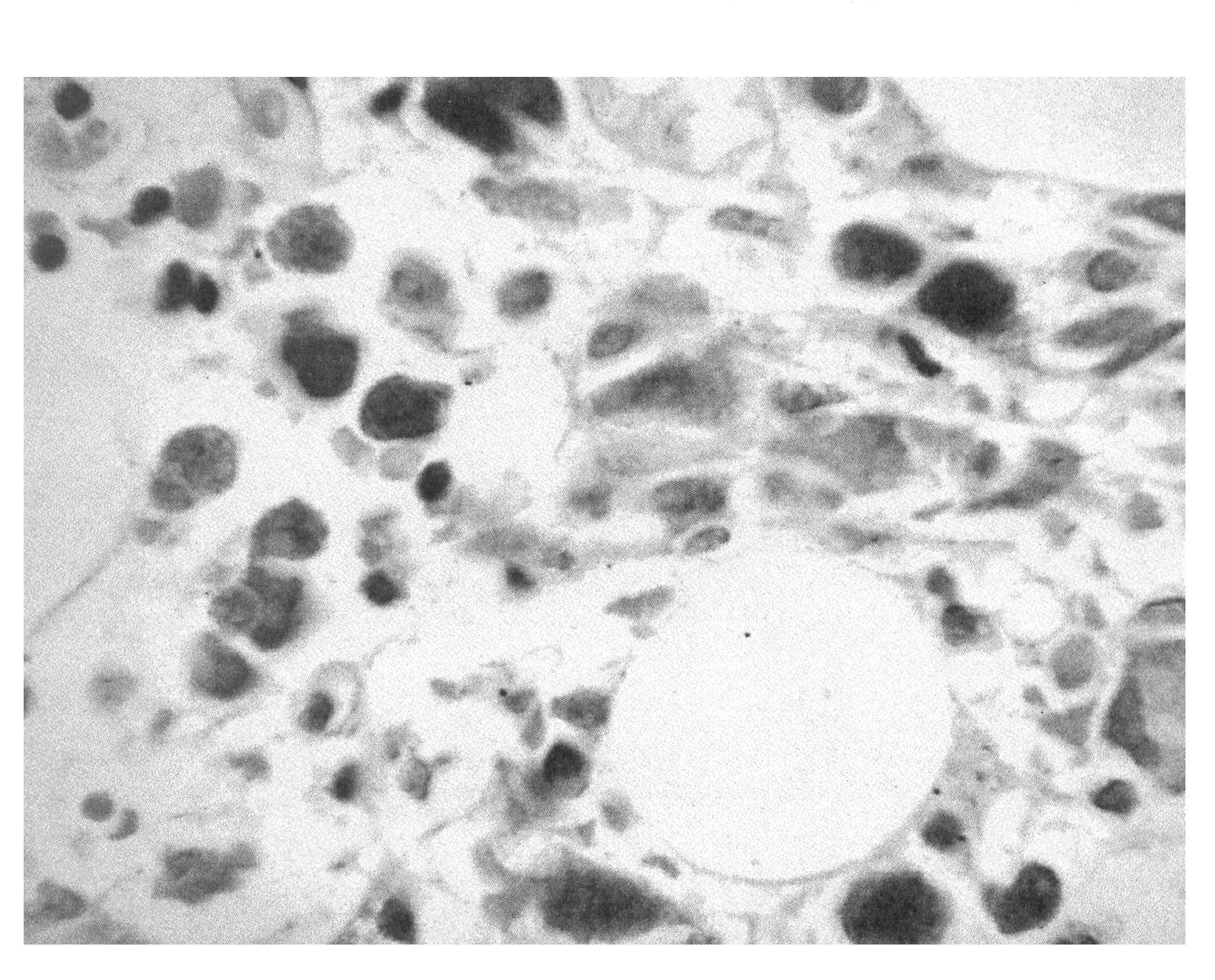
The patient was started on 4-drug induction using prednisone, vincristine, L-asparaginase and daunorubicin. On day 4 of induction he developed neutropenic fever with mucositis which was treated with antibiotics and antifungals. However, pancytopenia was persistent and the patient succumbed to his disease on day 35 of induction chemotherapy. Bone marrow examination at day 30 showed 70% blasts predominantly comprising larger blasts with similar morphology as described earlier along with mature lymphocytes; cellularity was 40% along with focal grade 3 reticulin fibrosis (Fig.1b). The smaller blasts as seen in the pre-treatment marrow were no longer seen suggesting that the lymphoid component had responded to chemotherapy.
Discussion Bilineal leukemias have two leukemic clonal populations of cells each expressing antigens of different lineages. They arise either denovo or following antileukemic chemotherapy and have poor prognosis. They can be suspected on morphology when two distinct populations of blast cells are present. The present case is unusual and unique on two aspects. Firstly, the lymphoid component is of T cell type and secondly it is in combination with a very rare megakaryocytic component. Such an unusual combination is difficult to diagnose without the aid of ancilliary techniques like imrnunophenotyping. According to the European group for immunological classification of leukemias criteria(3) for diagnosing acute biphenotypic leukemias, CD2 carries a score of one and megakaryocytic markers are not represented in the scoring system. Although the lymphoid score in our case was <2, the fact that they were morphologically lymphoid blasts with PAS positivity which disappeared in post chemotherapy repeat bone marrow smears suggests that they were lymphoblasts unequivocally. Further, CD41 positivity in larger blasts and accompanying fibrosis points strongly in favor of megakaryocytic lineage. CD2 has been reported to be coexpressed by megakaryocytic blasts in about 23% of cases(4); however, in our case the CD2 expression was demonstrated on morphologically distinct lymphoid blasts. In view of the large megakaryoblasts, morphologically it may sometimes be difficult to differentiate it from other round cell tumors like neuroblastoma, rhabdomyo-sarcoma which are of common occurrence in this age group; this underlines the importance of immunophenotyping. Contributors: US: writing the manuscript and performed laboratory studies; RS:: supervised laboratory studies and SB: writing the manuscript and patient care. Funding: Routine diagnostics. Competing interests: None.
| ||||
|
References | ||||
|
2. Matutes E, Morilla RM, Farahat N, Carbonell F, Swansbury J, Dyer M, et al. Definition of acute biphenotypic leukemia. Hematologica 1997; 82: 64-66. 3. Bene MC, Castoldi G, Knapp W, Ludwig WD, Matutes E, Orfao A, et al. Proposals for immunological classification of acute leukemias, European group for immunological classification of leukemias (EGIL). Leukemia 1995; 9: 1783-1786. 4. Athale UH, Razzouk BI, Raimondi SC, Tong X, Behm FG, Head
DR, et al. Biology and outcome of childhood acute
megakaryoblastic leukemia:a single institute experience. Blood
2001; 97: 3727-3732. |
![]()