|
|
Personal Practice Indian Pediatrics 2007;44:531-539 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Postnatal Corticosteroids for Chronic Lung Disease (CLD) |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
M. Jeeva Sankar From the Division of Neonatology, Department of Pediatrics, All
India Institute of Medical Sciences, Correspondence to: Dr. Ashok Deorari, Professor, Department of
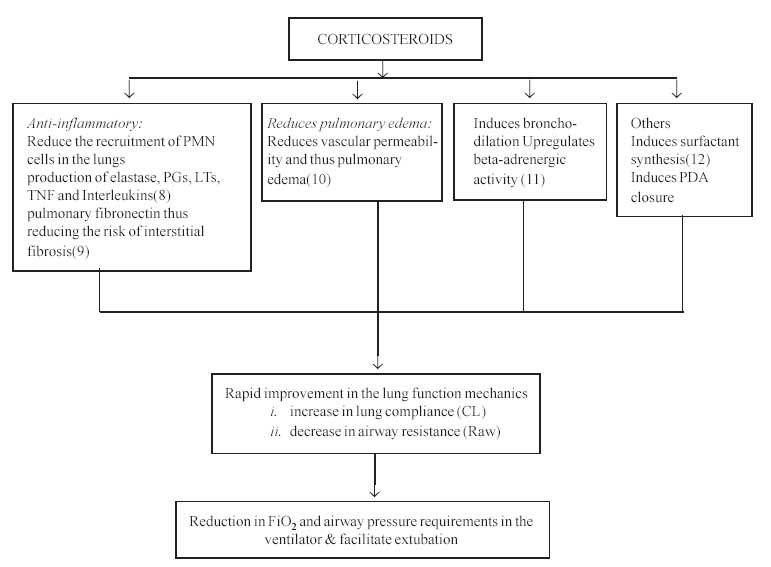
Pediatrics, All India Institute of Medical Science, Introduction Few topics in the field of neonatology have generated such a controversy as that on the use of postnatal steroids in chronic lung disease (CLD). Initially introduced with much enthusiasm, the use of postnatal steroids has snowballed into a controversy following recent reports of adverse neurodevelopmental outcomes. In this article, we shall review the risk-benefit ratio of postnatal steroid treatment and the evidence on the impact of steroids on brain development in preterm infants at-risk for CLD. Chronic Lung Disease It is almost 40 years since Northway first described the features of CLD, also referred to as bronchopulmonary dysplasia (BPD)(1). Classically defined as the need for supplemental oxygen(O2) at 28 days of age, now most consider a need for supplemental O2 at 36 weeks postmenstrual age (PMA) to be the reasonable indicator of BPD(2,3). According to two large data bases in Canada and in United States, the incidence of CLD among the surviving very low birth weight (VLBW) infants was 26% (1996-1997) and 23% (1995-1996) respectively(4,5). The only published study from India found the incidence of CLD to be 9% and 50% in VLBW and ELBW infants respectively(6). With increasing survival of smaller and more immature infants, the incidence of CLD is bound to increase. Rationale behind the use of steroids in BPD BPD occurs following exposure of immature lungs to high O2 concentrations and positive pressure ventilation. The resulting injury and inflammation lead to abnormal reparative processes seen in bronchopulmonary dysplasia(7). Since inflamma-tion plays the central role in the pathogenesis of BPD, it seems quite logical to use corticosteroids. The various mechanisms by which steroids could favorably influence the evolution CLD are summarized in Fig.1.
Steroids for CLD 1. Historical overview The first study of postnatal steroid (PNS) treatment was published as early as in 1956(13). The first randomized controlled trial (RCT) by Baden in 1972 evaluated the effects of steroid therapy on the evolution of infants with RDS but did not find any advantage when compared with placebo(14). Subsequently, Mammel and Avery in two separate RCTs demonstrated a significant improvement in lung function with faster weaning from mechanical ventilation in infants treated with steroids(15,16). This was followed by numerous RCTs in the 1980s and early 1990s(17-20). Except for a few studies, most were associated with shorter times on oxygen and mechanical ventilation and/or reduction in the incidence of BPD. Following these observations and also with the recognition of the importance of inflammation in the pathogenesis of CLD, postnatal steroids became the mainstay for treatment and even prevention of CLD. 2. PNS: Review of literature The use of steroids in CLD was thought to be one of the most robust, evidence-based therapies in neonatology until the follow-up data of treated infants became available. At least 48 RCTs have been conducted till date. Notwithstanding the heterogeneity of these trials, here is a summary of the common features of them. (a) Drug: With few exceptions, most of the studies including the last published trial (DART study) have used only dexamethasone(17-21). This is interesting given that betamethasone is preferred over dexamethasone for antenatal steroid treatment(22). (b) Route: Most studies have employed parenteral (intravenous) route. Because of the significant side effects associated with systemic therapy, several groups have attempted the use of inhaled steroids in infants with CLD(23-25). One of the major problems with this mode of administration was the difficulty and large variability in drug delivery to the distal portions of the lung. This may explain the variability of the results reported with inhaled steroids(26). (c) Timing: Postnatal steroids have been used either for prevention of CLD or to treat it once established. Based on the timing of initiation of the treatment, it can be categorized into 3 broad groups as follows: (i) Early treatment, during the first 96 hrs after birth; (ii) Moderately early treatment, between postnatal days 7 and 14; (iii) Delayed treatment, given after 3 weeks of age(27). (d) Dose and duration: Various studies have used different regimes for postnatal steroid treatment. The most commonly used regimes are summarized in Table I. TABLE I Dose and Duration of Postnatal Steroids Used in RCTs
*mode (range); PMA: postmenstrual age. 3. PNS: Outcome measures The Cochrane Neonatal Review Group (CNRG), which provides the most valid and reliable evidence on which to base decisions concerning treatment, has published 3 meta-analyses by incorporating all the controlled trials of postnatal steroids for CLD(28-30) (Table II). TABLE II Outcomes of PNS Treatment in Preterm Infants
*Significant effect; PMA: postmenstrual age; IVH: intraventricular hemorrhage. (From Halliday HL, Ehrenkranz RA: Cochrane Database Syst Rev 2003; (1): CD001144-46; reproduced with permission from the author) (a) Beneficial outcomes All the three regimes significantly reduce the incidence of combined outcome of death or CLD at 36 weeks PMA and also facilitate early extubation by 7th day after commencing steroid treatment. While both early and moderately early steroid therapy reduce the incidence of CLD at 36weeks PMA, late steroid therapy reduces the need for home oxygen therapy. However, they do not have significant effect on mortality alone (Table II). (b) Short-term side effects Infection, hyperglycemia, hypertension and GI bleeding are either significantly increased or show a trend towards increased incidence with early and moderately early steroid therapy (Table II). Growth failure is seen with both early and late steroid therapy. The incidences of severe intraventricular hemorrhage (IVH), periventricular leucomalacia (PVL) and necrotizing enterocolitis (NEC) are not significantly increased with steroid therapy (data not shown). (c) Long-term adverse effects There has been a major delay in the detection of the effect on neurodevelopmental outcome, the most controversial aspect of PNS, because (i) most studies have not looked for such an effect; (ii) few studies who have looked for that are underpowered to detect any difference; (iii) of the result of ‘contamination’, i.e., use of open-label steroids in the control group (up to 62% in some studies)(16); (iv) of the heterogeneity in the study population, timing and dosage of PNS, time of assessment and the instruments used to assess neurodevelopment. Two systematic reviews are available that focus on long-term neurodevelopment of infants following PNS treatment(31-32). In one review of 5 trials, motor dysfunction was found to be significantly greater with steroid treatment while mortality was not different(31). Barrington KJ performed a systematic review by identifying 3 additional trials that reported on the long term outcome after postnatal steroid treatment(32). These 8 studies represent 1052 infants; 292 of them died and 679(89%) of the 760 survivors were followed for 1 year or longer. He tried to address the effect of contamination by arbitrarily dividing the studies into 2 groups on the basis of whether they had <30% contamination [Group 1] or >30% contamination [Group 2]. The outcomes evaluated were the incidences of cerebral palsy and neurodevelopmental impairment defined as a developmental score more than 2 standard deviations (SD) below the mean or cerebral palsy or blindness. The results are summarized in Table III. TABLE III Meta-analysis of Effects of PNS on Neurodevelopment
* Significant effect; (From Barrington KJ. The adverse neuro-developmental effects of postnatal steroids in the preterm infant: a systematic review of RCTs.) (32). Thus, the infants who received PNS were twice as likely to develop cerebral palsy as the control infants. Similarly, steroid treated infants have 1.34 times the risk of having neurodevelopmental impairment. This apparent effect increases as the degree of contamination reduces between the two groups (RR of 2.89 and 1.66, respectively) implying that ‘open-label’ use of steroids in the control group reduced the apparent size of adverse effects noted with steroid therapy. Since there was no effect on mortality between the 2 groups, it was calculated that the number needed to harm (NNH), with regard to the incidence of cerebral palsy, is 7. In other words, for every 7 infants treated with postnatal steroids, there will one additional surviving infant with cerebral palsy(32). These results, however, have been criticized by various authors who question the impropriety of combining eight heterogeneous studies to assess the neurodevelopmental outcome(33). At least three additional trials that reported long-term outcomes have been published since the review by Barrington. These studies yield conflicting results; because of the heterogeneity in the study populations, timing and dosage of steroid treatment, the data could not be combined using meta-analytic techniques(34-36). Recently, Watterberg, et al. studied the long term outcomes of ELBW infants following early Low-Dose Hydrocortisone and found that hydrocortisone was not associated with an increase in CP and indeed had indicators of improved neurodevelopmental outcome(37). However, a Benchmarking Subcommittee of the National Institute of Child Health & Human Development (NICHD), that looked for the impact of PNS in ELBW infants found that for each 1 mg/kg PNS dose (95% dexamethasone), mental development index (MDI) decreased by 2.0 pts (p<0.0001) and disabling CP increased by 40% (OR 1.4, 95 CI 1.2-1.6). They concluded that increased PNS dose was associated with increased neurodevelopment impairment (E-PAS 2006:59:4355.6). Scientific background for adverse neurodevelopmental outcome Conflicting data from clinical studies raise the possibility of a direct neurotoxic effect of steroid therapy. Supporting evidence has emerged from laboratory models together with imaging studies of the human brain. 1. PNS and gross brain development Experiments with newborn rodents indicate that steroids can cause a substantial decrease in brain weight(38). Human studies have shown reduced head growth (as determined by occipitofrontal circumference) and cerebral cortical gray matter volume (as determined by volumetric 3-dimensional MRI technique) in preterm infants treated with dexamethasone(39-40). 2. PNS and neuronal proliferation & maturation PNS has been proved to impair both brain cell division and myelination(41). Studies in mice have shown that steroids interfered with the synthesis of DNA, RNA, and protein in the brain with irreversible reductions in the cell number(38). In the human brain, neurons in certain areas like hippocampal dentate gyrus continue to divide long after birth and hence remain vulnerable to these adverse influences(27). The effects on myelination might explain the long-term behavioral disturbances seen following PNS. The mechanisms by which steroids affect brain growth remain unclear, but the possible theories are (a) inhibition of growth factors and facilitation of apoptosis(42). (b) by modifying the properties of NMDA glutamate receptors that lead to neuronal cell death following the release of glutamate(43). (c) due to the effect of neurotoxic sulphite preservatives present in injectable preparations of dexamethasone. Sulphites have excitotoxic like properties and may play a key role in steroid induced brain damage(44). It is interesting to note that injectable betamethasone does not contain this preservative. PNS: Role of inhaled steroids Several groups have attempted the use of inhaled steroids in infants with impending or established CLD(23-25). Two systematic reviews address the effectiveness of inhaled steroids to prevent CLD in VLBW infants(45-46). No benefit of inhaled steroids was shown. Another two systematic reviews that evaluated the role of inhaled steroids for treatment of evolving CLD in ventilator dependent VLBW infants found that there was no evidence of difference in effectiveness or side-effect profiles for inhaled versus systemic steroids(45,47). Postnatal steroid treatment: Current scenario Following reports of potential adverse effects, the initial enthusiasm surrounding steroid use turned into fear finally culminating in the publication of restrictive guidelines. 1. Policy statement: AAP and Canadian Pediatric Society, 2002 In view of the concerns regarding short and long-term adverse effects and the uncertainty regarding the short and long-term benefits, the Committee on Fetus and Newborn of American Academy of Pediatrics (AAP) and Canadian Pediatric Society (CPS) came up with a policy statement in 2002(48). The salient features of this statement are (a) The routine use of dexamethasone for prevention or treatment of CLD in VLBW infants is not recommended. The use should be limited to carefully designed RCTs that have neuro-developmental outcome as part of their protocol (b) Outside the context of RCTs, the use of steroids should be limited to exceptional circumstances (c) There should be full informed consent of the family regarding the potential short- and long-term risks of steroids. 2. AAP policy statement: Controversy Since their publication, the guidelines have continued to spark disagreement among neonatologists. While some opine that the risk-benefit ratio for moderately early and late therapy is reasonable and there is no need to restrict, others feel that limiting their use to ‘exceptional circumstances’ would result in delay in therapy to an age when the infant is less likely to respond(49). Not withstanding these objections, the use of postnatal steroids has declined significantly in North America. A prospective study in 2003 showed that steroid use for non-CLD indications was significantly greater than that for CLD use (11.8% vs 7.6%)(50). To date, there are few data regarding the effects at a population level of this change in therapy on the incidence of mortality or CLD(51). Postnatal Steroid Treatment: Indian Scenario Even after years of extensive research, there are no proven safe and beneficial therapies available to prevent or treat CLD(52). In developed countries, the emphasis is now clearly on supportive management in the form of aggressive parenteral nutrition and ‘gentle ventilation’(7). In India, where the supportive management of VLBW infants is sub optimal in many neonatal units, there are hardly few studies available in this regard. Also there are no guidelines regarding the use of postnatal steroids for CLD. Despite the risk, though not convincing for adverse long-term outcomes, use of postnatal dexamethasone may still be warranted to facilitate early extubation in ventilator dependent ELBW infants (‘exceptional circumstances’). After a careful review of the available literature, the following recommendations seem reasonable for the use of steroids in CLD. (Table IV). However one has to remember that these are, at best, empirical and not evidence-based. TABLE IV Recommendations for PNS Therapy for CLD*
* Empirical and not evidence-based; Parents should be fully informed of the potential adverse outcomes Implications for research With increasing survival of smaller and more premature babies, it is essential to have a very low birth weight (VLBW) registry in India that would help in creating a huge database which would give essential information regarding the selected morbidities and mortality of these infants. Also, properly conducted studies are needed to assess the effectiveness and side effects of the recommended low-dose short-duration dexamethasone therapy in Indian infants. Conclusions With increasing survival of VLBW babies, the incidence of chronic lung disease is also bound to increase. Till now, there are no effective and safe options available for treatment of CLD. The role of postnatal corticosteroids in chronic lung disease is still controversial. Its use, though associated with short-term benefits, does not alter the long term pulmonary outcome. Also, there are serious concerns regarding the adverse neurodevelopmental out-comes following its use. Notwithstanding such an effect, there might be still be a role for postnatal steroids (albeit, in low doses), especially in ELBW babies who are ventilator dependent even after 14 days of ]age. There is an urgent need for well conducted RCTs to study the effects of such regime in Indian babies. Contributors: JSM reviewed and drafted the paper. AKD provided overall framework and concept; he will act as the guarantor of the article. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()