|
|
Case Reports Indian Pediatrics 2005; 42:708-710 |
||||||||||||||||||||||||||||||||||||||||||||||
|
Anterior Urethral Valves |
||||||||||||||||||||||||||||||||||||||||||||||
|
From the Department of Pediatric Surgery, Post Graduate Institute of Medical Education and Research, Chandigarh 160 012, India.
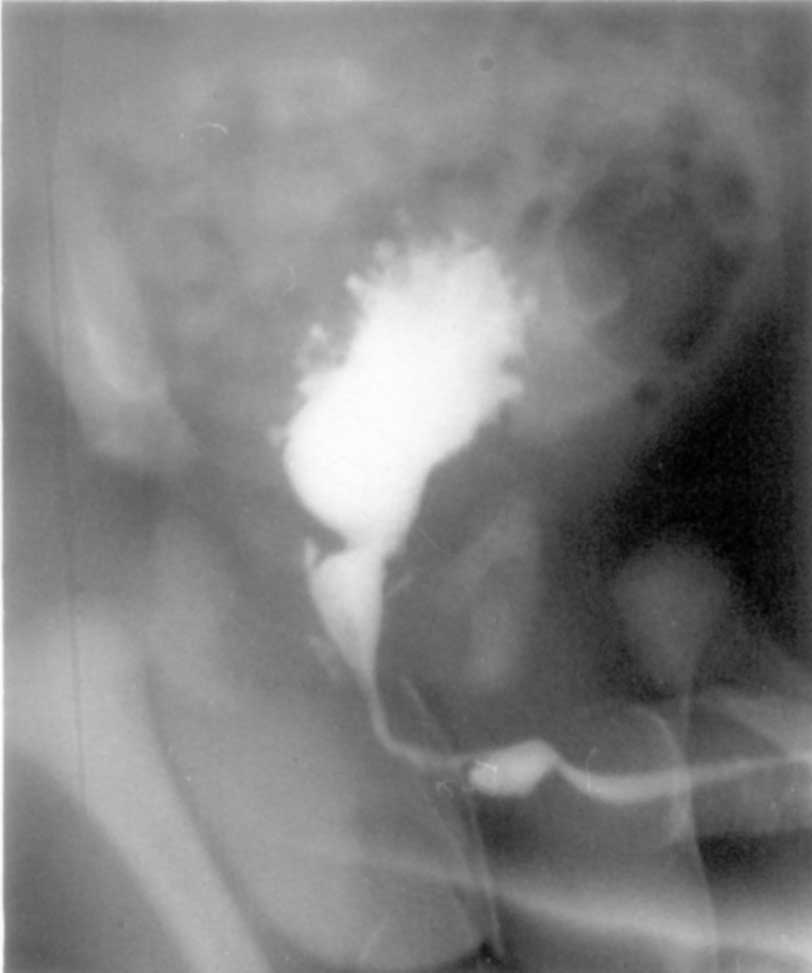
Cases Of 264 boys with obstructive uropathy presenting at this center between 1989-2004, 246 had PUV. Five patients had anterior urethral valves (Figs.1,2). The clinical details of these patients are given in Table I. TABLE I Clincial features and outcome in patients with anterior urethral valves
One patient presented with antenatally diagnosed bilateral hydronephrosis and oligohydramnios (Pt. 4). One patient had associated perineal bulge and urethral diverticulum with anterior urethral valves (Fig. 2, Pt. 5). Two patients had associated grade V vesicoureteric reflux. The site of obstruction was the penoscrotal junction in 4 and root of penis in one patient. All cases were successfully treated endoscopically.
Discussion Anterior urethral valves are rare causes of obstructive uropathy in boys with only three large series(1,2,5). They are an important cause of urinary tract obstruction in children and can be easily missed by an unaware clinician(3,4,6). They occur less frequently than PUV. Anterior urethral valves are congenital in nature and can be located anywhere in the anterior urethra viz., approximately 40% in the bulbar urethra, 30% at the penoscrotal junction and 30% in the penile urethra. Some of them exist without an associated diverticulum(2). Four of the 5 patients in this report presented without an associated diverticulum. The clinical presentation of anterior urethral valves is similar to that of PUV. The spectrum ranges from mild urethral dilatation to bilateral hydronephrosis with renal insufficiency. Anterior urethral valves can cause histological changes in the bladder similar to PUV and produce valve bladder like picture(1-6). The presentation in the developed countries is usually as an antenatally diagnosed hydronephrosis because of routine antenatal screening. However, in our country the presentation is usually seen in older children with obstructive urinary symptoms, and/or urinary tract infections. It is estimated that one third of patients with anterior urethral valves have an associated diverticulum, which presents as a swelling in the root of the penis after voiding and compression of which results in dribbling of urine from the meatus(2). Fewer than 5% of the patients with anterior urethral valves progress to renal failure. Patients with significant upper tract deterioration present at a younger age(2). It is recommended that a MCU be done for diagnosis, since the valves are likely to be missed on retrograde urethrography, as they remain open with retrograde flow(1-3). The whole of the anterior urethra must be included in the field of exposure while doing MCU in order to avoid missing the site of obstruction. Baseline renal functions and follow up must be done like PUV. Approximately one-half of all patients can be treated with simple transurethral fulguration. Savage, et al. have proposed an algorithm for treatment based on the severity of disease(2), which recommends vesicostomy in infants with high grade reflux and poor emptying of the urinary tract. If the urethra is of sufficient caliber and support, transurethral fulguration is recommended. Open urethroplasty is useful in patients with a large urethral diverticulum and thin urethra. Contributors: KLN, SKC, BK worked up the case and collected the literature; KLN will act as guarantor. Funding: None. Competing interests: None.
| ||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||
|
|
![]()