|
|
Special Article Indian Pediatrics 2005; 42:653-663 |
||||
|
Understanding and addressing Childhood Immunization Coverage in Urban Slums |
||||
|
Siddharth Agarwal,
Introduction The National Population Policy (NPP), 2000 aims to immunize all children against six common childhood diseases (tuberculosis, tetanus, pertussis, diphtheria, measles and polio) by 2010. Although immunization coverage has increased substantially in recent years, large numbers of slum dwelling children remain incompletely immunized(1). The urban# poor, many residing in slums, comprise about one-fourth of India’s 285 million urban population(2).
Present scenario in urban India Among children aged 12-23 months in urban India, 60% are fully immunized (immunization cards and mother’s recall) which presents an average of the better and poorly performing states. Empowered Action Group (EAG)† states which constitute more than 40% of the total urban population of India(2) are way behind. Immunization coverage in urban areas of Bihar, Rajasthan and Orissa is 19%, 27% and 49% respectively as compared to 84% and 73% in Tamil Nadu and Kerala(3). Immunization services do not reach over one third of urban poor children; only 43% are fully immunized(3). The percentage of children completely immunized in the low as compared to high SLI (Standard of Living Index is representative of socio-economic status) in urban areas is 7 versus 53 in Rajasthan and 24 versus 76 in Orissa. This difference is less marked in better performing states like Punjab and Kerala. Slum based studies confirm this finding(4,5). Such interstate differentials indicate the importance of extra focus on lower performing states. "Heightened" importance of childhood vaccination in urban slum settings Outbreaks of Vaccine Preventable Diseases are more common in urban slums owing to high population density and continuous influx of a new pool of infective agents with the immigrating population(6,7). Measles produces a higher percentage of younger cases with associated higher mortality, owing to prolonged exposure to infected siblings in the small living space of slums. Severity of infection is higher in these secondary cases(8). Immunization programs in urban areas can exert significant effects on vaccine preventable disease associated mortality by limiting the number of cases, decreasing clustering of cases within households and increasing time lapse between outbreaks(9). There is growing recognition that the responsibility of pediatricians has to expand beyond providing clinical care, to ensuring child survival, health and development. Pediatricians thus have a pivotal role in reaching out to urban India’s forgotten children with the efficacious, simple and cost effective intervention of immunization. In light of the emphasis on strengthening immunization services in underserved urban areas by National Technical Advisory Group on Immunization (NTAGI)(10) and the IAP theme for 2005 "Extra care for children of urban poor and migrating population"(11) this article examines issues and suggestions for improving immunization coverage in urban slums. Problems and challenges in routine immunization coverage in urban slums
Urban primary care facilities till late 1990’s were grossly inadequate with only one UFWC/HP per 145,854 urban popula-tions(12). Through India Population Project (IPP) VIII (1993 to 2002) 531 new facilities were constructed and 661 facilities were upgraded/renovated in Bangalore, Delhi, Hyderabad and Kolkata(13). However, the program did not reach all urban poor even in these cities. Absence of a well plotted city map indicating slums and facilities leads to crowding of several primary care facilities in a small area of the city, usually its centre. Further weak coordination may result in duplication of services in some areas, particularly in mega cities. Staffing has not increased in response to urban growth(14). Low staff motivation owing to weak public transport system, lack of supportive supervision among other reasons results in weak outreach(15).
Immunization services scarcely reach non-recognized slums while notified slums may receive benefits of repeated interventions(16). Some slums are situated on the border of two Urban Family Welfare Centers (UFWCs) / Health Posts (HPs) with neither of the facilities taking responsibility for these (17,18). Similarly, neither rural nor urban health staff takes ownership of periurban slums. Certain population segments remain "hidden" due to their temporary or migratory nature (19,20).
The absence of the Roseto Effect(21) or lack of social fabric in urban slums often limits interpersonal interaction and information about services. Urban poor are often not able to muster enough confidence to access services even when services are proximal. Working mothers do not get the support required to attend to child’s health needs when they are occupied in livelihood generation activities. (iv) Inadequate demand for services among urban poor populations The demand for immunization services requires acceptability for immunization that is, clear understanding of benefits, no fear of vaccines, specific knowledge of vaccine doses, motivation to avail services and overcoming barriers for seeking immunization services(22). Evidence suggests that poor uptake of immunization in urban areas is associated with mother’s unawareness about repeat visits to achieve complete immunization rather than overall vaccine aware-ness(23). Slum dwellers are unable to demand services owing to weak community organization and low collective confidence which is known to increase utilization of health services(24). In the absence of outreach activities or difficulty in availing these services due to camp timings as in the case of working mothers, fixed facility are rarely used for availing immunization services. In certain slum populations religious and traditional beliefs prevent receipt of available immunization services.
The birth registration system particularly for urban slums is very weak. Many domiciliary deliveries which are as high as 85.3% and 79% amongst urban poor in Uttar Pradesh and Rajasthan(3), remain non-registered. Monitoring of service quality, reach and age appropriateness of immunization coverage is rarely used as a tool to improve performance. In EAG states, half the urban poor children who begin their immunization series drop out. (vi) Program planning and protocol related issues Routine immunization program is caught in a "Development Dilemma". It faces competition from well funded, top-down, and short term disease specific initiatives(25). National events (such as pulse polio campaign) divert service providers’ efforts away from routine immunization activities. Often planners and service providing personnel harbor the perspective that slums are ‘illegal’ and providing them services implies giving them legal sanctity. (vii) Missed immunization opportunities in slums There are "missed opportunities" when medical practitioners who are consulted for childrens’ ailments do not provide immuniza-tion services or related counseling(26). There is a tendency among providers to wait for an optimum number of children to arrive at the outreach camp before opening a multi dose vial such as measles or BCG(15). Also, health workers are yet to muster confidence for administering two or more vaccines on the same visit, even though there is no contraindication or loss of efficacy in administering multiple vaccines provided they are administered at different sites(27,28). Despite a positive attitude towards immunization child may not get immunized during minor ailments, owing to family members’ apprehensions, even when illness is not contraindicative to immunization(29,30).
There may be underestimation and consequent insufficient supply of vaccine quantity for outreach camps(31,32). In many instances injuries and infection caused due to wrong injection procedures and the negative attitude of service provider are discouraging for care- takers(33). The absence of systems of safe disposal of injection sharps and plastics such as shredding and disinfection(34) may lead to dumping of waste material at camp sites, exposing slum children to risks. Though not directly related to utilization of immunization services safe disposal of immunization wastes is an imperative health concern, particularly for rag-pickers who may cut themselves on needles and pieces of glass in the garbage, which may expose them to infections. Child rag pickers face a greater threat of occupational hazards and injuries due to their lack of judgment, experience and knowledge(35). Opportunities and options Seeing the glass half full or half empty; crowded living of slums makes larger number of people geographically accessible for outreach activities in lesser time unlike rural areas where population is more dispersed. Physical access to health facilities is not a major obstacle.There are more options for IEC and related communication activities. Resources and potential partners abound: Municipal, Health Department, NGOs, Private and Charitable hospitals, amongst others. Integrated Child Development Services (ICDS), where present has a greater impact on immunization coverage in urban slums than rural areas(36). Since a sizeable urban poor population approaches non-qualified practitioners for curative care there is a growing view of involving them to counsel caretakers on timely immunization as well as training them to provide routine immunization services. In the wake of the 74th amendment to India’s constitution, the Urban Local Bodies (ULBs)*(37) when adequately stimulated will own the effort since it would help the elected representatives in nurturing their constituency. There has been growing recognition of the problem of urban slum dwellers among Government agencies, donors and NGOs. Urban health has been recognized as an important focus area in the Tenth Five Year Plan for which a separate budget (Rs. 700 crore) has been allocated.
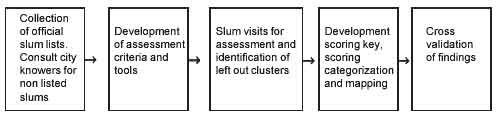
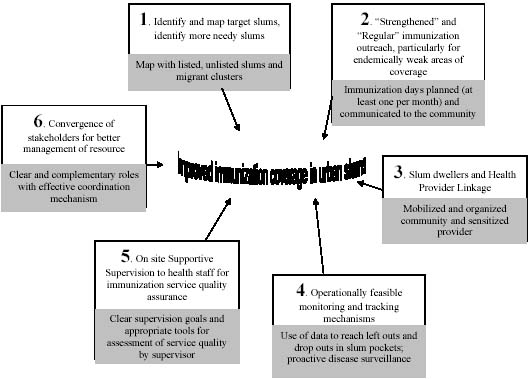
The way forward Achievement of universal childhood immunization by 2010 requires reach of services to urban poor through effective outreach and optimum use of fixed facilities. Six key processes to improve immunization coverage in urban slums are suggested. Process 1: Identify all slums; use mapping and vulnerability assessment of slums as a planning tool Mapping of all slums, beyond official lists with the help of "city knowers" and slum assessment using inclusive criteria of vulnerability(38), enables identification of endemically weak areas of immunization coverage. Some urban slums were among the most difficult to reach areas during Pulse Polio campaign through recent experiences(39). Catchments of primary level facilities can be redefined based on city maps to ensure reach to left out pockets and equitable distribution of work. Where infrastructure is inadequate the need for new facilities will clearly emerge from the map. An approach for identifying unreached target groups based on the EHP’s experience in 6 cities: Dehradun, Haridwar, Haldwani, Bally (West Bengal), Jamshedpur, Agra is outlined in Fig. 1.
Process 2: "Strengthened" and "Regular" immunization outreach, particularly for areas with poor access Organizing an effective immunization outreach camp An immunization session is effective only if each child and woman attending it receives all vaccines s/he is eligible for, following necessary safety and efficacy procedures and returns timely for the next vaccine(40). Regular outreach camps at a convenient, well publicized, preferably fixed location and day, for the pre-informed time by health staffs, with support from local stakeholders are essential in endemically low coverage urban areas. This requires micro planning with Ward or Urban Health Center (UHC) forming the unit for planning(39). A functional linkage between the ANM and AWW or community health volunteer with support from medical officer or Lady Health Visitor enables identification and registration of pregnant women, new births and children <5 years of age through a quick mapping of lanes and houses in the slum and its monthly updation. Caution should be observed in not limiting this list to the beneficiary list as per ICDS criteria. ULBs can contribute financial or in kind support (such as transport, camp logistics, publicity) for immunization activities through various schemes and programs namely Swarna Jayanti Shahri Rozgar Yojna (CDS and Development of Women and Children in Urban Areas - DWCUA) and National Slum Development Program (NSDP). Community Halls developed by DUDA, private/ government schools, private doctors’ clinics, angan-wadi centers, community worship areas and other approachable venues may be used as site for immunization camps. Pediatricians in public and private sector can provide training for effective immunization outreach sessions and support monitoring of such camps. Immunization focused publicity and social mobilization Mass media immunization drives where urban slums have better access to such media(24) combined with community counseling and peer contact(41,42) can enhance service utilization. Communication should be targeted to move caretakers from inertia i.e., fear of vaccine and no fear of disease to action i.e., no fear of vaccine and fear of disease(43). Community’s concerns towards immunization should be addressed through involvement of decision makers like father, mother-in-law in addition to the mother and anti-vaccine rumors need to be countered(44). Health workers should counsel caretakers encouragingly and persuasively to avail immunization services when giving the immunization card. For areas predominantly occupied by migrating population announcement of immunization days and venue through loudspeakers is effective. Pediatricians and general medical practitioners could distribute pictorial cards or leaflets indicating appropriate age for different vaccines and reinforce significance of timely immunization when children visit for consultation. These will encourage families for getting children immunized even when they migrate to other areas. Process 3: Slum dwellers and Health Provider Linkage Community participation improves vaccination coverage(22, 45). However, more pressing issues of insecurity and disabling environment often undermine a slum dweller’s motivation to ensure immunization for children. Sanchetna, an Ahmedabad based voluntary organization has successfully trained slum women as community health workers (CHWs) to improve outreach and referral to clinics(46). A similar strategy has been effective in IPP VIII program in West Bengal, Andhra Pradesh, Bangalore and Delhi. A ‘link volunteer’, essentially a resident slum woman trained on health issues and equipped with referral cards, has been proposed in Government of India’s Urban Slum Health Guidelines for RCH II(47). Process 4: Effective monitoring and tracking mechanisms An effective monitoring and tracking mechanism enables identification of catchment areas of low reach, operational problems in improving coverage and corrective action to enhance service utilization. Both quality of immunization activities (i.e., ensuring adequate supplies, vaccine efficacy, correct administration, post administration counseling, safe disposal of immunization wastes) and outcomes (immunization reach, identification and follow-up of left outs# and drop outs*) need to be monitored(48). Impact assessment through disease surveillance is also necessary.
Assessing quality of immunization services: An observational checklist of quality criteria may be used for supportive supervision by Medical Officers or a trained supervisor through random visits to immunization outreach camps and fixed facilities. The ANM or trained Community health worker, having first hand understanding of field realities can effectively monitor outcomes, analyze problems and identify solutions. Periodic monitoring of immunization coverage and disease surveillance: Developing graphs using monthly immunization coverage data by Medical Officer, LHV and ANMs is a vital tool for assessing effectiveness of immunization camps. Disease Surveillance: Monthly reporting of VPD cases by the ANM during outreach activities as well as at the fixed facility needs to be revitalized and regularly monitored. A decrease in the incidence of VPDs over time is important to ensure that immunization services are effective. Slum level tracking mechanism: In the EHP supported urban health program in Indore, Community Based Organizations (CBOs) compile information and distribute "family chits" providing name, date of birth, address and immunization eligibility of the child for the upcoming camp in selected slums. The counterfoil is retained by the CBO which helps in confirming timely immunization. Once the family is inducted the child’s attendant receives the chit for the next immunization at the preceding camp. Process 5: Supportive Supervision for immunization service quality assurance Low motivation of health staff due to unduly large catchment area, lack of recognition, appropriate guidance and effective management systems contributes to the overall inability to reach all eligible children. Supportive supervision with defined goals and tools, to ensure quality and optimum reach of immunization services at outreach camps and health centers, is vital. Supervisor should be trained in facilitative supervision that emphasizes two-way communication, coaching, mentoring and joint problem solving(49,50). Medical professionals providing pediatric services should adapt such approaches to suit their operating context and enhance motivation and effectiveness of health workers.
Process 6: Convergence of stakeholders for better resource management Urban health stakeholders include Health and Family Welfare Department, Municipal Corporation, Urban Development Authority, ICDS, NGOs, CBOs, donor agencies, professional bodies (IMA, IAP), private sector (Private providers–formal and informal, Corporates), Employees State Insurance, religious leaders, local resources such as schools and the slum people themselves. Multi-stakeholder coordination planning at city level can optimize use of such diverse resources and involves: • Formation of a coordination forum with representation of all stakeholder groups and identifying complementary roles based on each stakeholder’s capacity. • Regular meetings of the coordination forum with defined plans and envisaged outcomes A multi-stakeholder coordination approach and synchronized activities were effective in the 1990 Universal Immunization campaign in Kolkata(41). Policy issues The proposed increase in government spending on health and education, with a focus on primary sector, in the Government’s Common Minimum Program (CMP) and universalization of ICDS can serve as an impetus to strengthening the immunization program(51). The slum level link volunteer proposed under RCH II (GOI’s Reproductive and Child Health Progam) will provide the much needed community-provider connection(47). An intensive, target driven plan is needed for the EAG states to catch-up with the better performing states. Considering occurrence of measles at an early age, and higher associated risk of mortality in urban slums, a sustained measles immunization campaign would be worth piloting in few of the most densely populated cities of India identified from GOI’s list of priority Common Minimum Program (CMP) districts and assessing its impact on measles related morbidity and mortality. Such a campaign should include (a) specific communication focused on measles immunization by 9 months and (b) special measles drives before seasons known for measles outbreaks. Caution should be observed that focus on the need of equitably high routine immunization coverage is not lost since coverage amongst urban low SLI population is only 43%(3). Conclusion Rapid growth, high population density and low immunization coverage in urban slums calls for growing emphasis on immunization coverage for vulnerable urban poor where spread of infection is faster. Available data on immunization and related indicators for the urban poor highlights inter state disparities and the need to prioritize EAG states when developing policies and programs for routine immunization. Universal immunization coverage as per Global Alliance for Vaccines and Immunization (GAVI) and National goals requires overcoming challenges of weak urban primary health infrastructure, "hidden" urban poor populations, poor social access, inadequate demand for services, weak monitoring and policy implementation issues amongst others. These goals can be reached through (a) effective outreach for underserved population and community empowerment to demand quality services; (b) utilizing available resources by multi-stakeholder coordination; (c) enhancing quality through improved supervision and joint problem solving; and (d) strengthened monitoring of left outs and drop outs. A national mission for taking immunization to the unreached will lend the much needed political, civil society and media pressure and periodic uproar on the issue. Acknowledgements The authors owe thanks to Robert Steinglass ImmunizationBasics for the detailed critical review of the manuscript. Thanks are due to Dr. Massee Bateman (USAID), Dr. Cherian (WHO) and Dr. HPS Sachdev for the technical information and support in developing this paper. The authors are grateful to Madhvi Mathur and Kaushik (EHP) for reviewing and editing the drafts and the program partners in Indore for sharing valuable pertinent information. This research was supported by USAID through the Environmental Health Project managed by CDM International Inc.
| ||||
|
References | ||||
|
|
![]()