|
|
Case Reports Indian Pediatrics 2002; 39:684-689 |
||
|
Primary Angiitis of the Central Nervous System |
||
|
Maina P. Kava
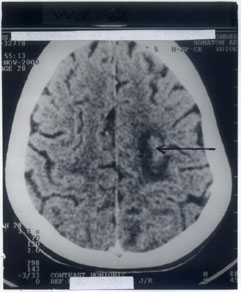
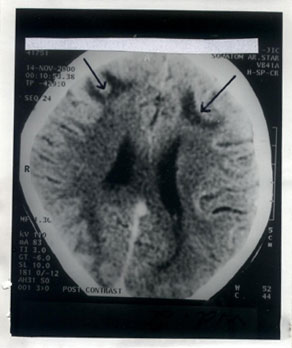
Primary angiitis of the central nervous system (PACNS) is a rare idiopathic disorder with recurrent vasculitis restricted to the central nervous system (CNS) and involves the small-sized (and at times the medium-sized) blood vessels(1,2). The typical clinical manifestations include multifocal strokes or encephalopathy, often associated with severe headache(3). There are very few pediatric cases with PACNS reported in the literature. The diagnosis of PACNS is mainly based on the clinical features, demonstration of angiitis on angiography or biopsy and exclusion of secondary causes of angiitis. A high index of suspicion is necessary for the diagnosis(4). Though the prognosis is generally poor, use of steroids and immunosuppressive therapy have been useful to achieve successful remission in many patients(1,4-7). We report a case of PACNS in a child with a brief review of literature. Case Report An eleven-year-old girl born of a third degree consanguineous marriage was brought with the complaints of fever and headache for two months and two episodes of left focal convulsions four days prior to admission. Her sensorium and vital parameters were normal and the general examination was non-contributory. CNS examination was normal except for papilledema on fundoscopic examination. After 12 hours of admission, she had one more episode of left focal convulsion associated with altered sensorium. Her sensorium showed a waxing and waning course over the next seven days. A computed tomographic (CT) scan of the brain after the first convulsion had shown a left parietal venous infarct (Fig. 1). A repeat CT scan after admission (after the third convulsion) revealed bilateral white matter changes with bilateral frontal infarcts (Fig.2). Complete hemogram, chest radiograph, sickling test, renal and liver function tests, prothrombin time and partial thromboplastin time were normal. Urine cyanide-nitroprusside test for homocystinuria was negative. Serological tests for human immunodeficiency virus and hepatitis B virus were negative. A cerebrospinal fluid (CSF) examination done on third day after admission revealed seven red blood cells, three lymphocytes and proteins of 70 mg/dl with normal CSF sugar.
Fig 1 Contrast CT scan of brain: Note the hypodense venous infarct in the left parietal region with peri-lesional edema (arrow)
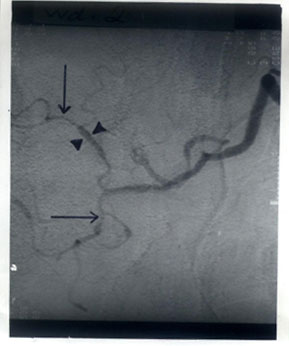
Fig 2. Contrast CT scan of brain: Note the bilateral white matter changes with bilateral infarcts in the frontal region (arrows) She was treated with a five-day course of intravenous methylprednisolone and ten days of intravenous acyclovir and antibiotics. Her sensorium showed some improvement but she was noticed to have quadriparesis with bladder and bowel incontinence on the tenth day of admission. A magnetic resonance angiography (MRA) of the brain suggested bilateral focal stenosis of the supraclinoid internal carotid arteries, proximal middle cerebral arteries, posterior cerebral arteries and terminal basilar arteries (Fig. 3). The digital subtraction angiography (DSA) showed focal areas of segmental stenosis and dilatation of the anterior, middle and posterior cerebral arteries with random involvement of all the intracranial vessels (Fig.4). Further investigations for vasculitis were performed. The protein C, protein S and antithrombin III levels were normal and the serum was negative for antinuclear antibodies, anti- DNA antibodies, rheumatoid factor, anti-cardiolipin antibodies, antiphospholipid antibodies and VDRL. The patient regained normal sensorium and bladder and bowel continence over the next week with gradual improvement in the muscle power. At discharge from the hospital after six weeks of admission, she had power of 2/5 in the upper limbs and 3/5 in the lower limbs. The patient was also started on treatment with oral prednisolone eight days prior to the discharge. After a month of follow-up, the patient showed remarkable improvement regaining her ability to stand with support. Treatment with oral prednisolone was continued. The patient did not follow-up further.
Fig. 3. MRA - brain: Note the bilaterial focal stenosis of the middle cerebral arteries(arrows).
Fig. 4. Digital Subtraction Angiography: Note the focal areas of segmental vessel stenosis (arrows) and dilatation (arrow heads) of the posterior cerebral arteries.
Discussion Primary angiitis of the central nervous system (PACNS), also described as isolated angiitis of the CNS, non-infectious granulomatous angiitis, cerebral granu-lomatous angiitis, etc. has variable and non-specific clinical manifestations referable to the CNS(1-4,6,8,9). PACNS is mostly seen in young to middle aged adults. The clinical features suggest presence of CNS ischemia in multiple areas of the brain(4). Gradual onset of severe and throbbing headache, features of dementia and later focal deficits can occur (1,3-5,7-9). Features of cortical dysfunction are frequent and may be accompanied by nausea and vomiting(8). Hemiparesis, dysphasia, cranial nerve palsies and extensor plantar responses can occur(1,4,8). Seizures, though uncommon in PACNS (observed in only 13% of cases), were present in our case(1,4,5). Multiple localized lesions of the cerebrum, cerebellum and brainstem are seen in over 75% of the cases(1). The clinical course may be rapidly progressive over days to weeks or insidious over many months with waxing and waning, or with clinical stabilization for a prolonged period(2,4). Isolated strokes, isolated spinal cord angiitis, chronic meningitis, papilledema, exptrapyramidal signs, brain-stem infarction and Korsakoff syndrome are rare(1,4,8). As in our case, there is relative absence of constitutional symptoms (like fever, loss of weight, myalgia, arthralgia, etc.) which suggest the presence of systemic vasculitis conditions with CNS involve-ment(1,4). The etiopathogenesis is not known, but herpes zoster infection, Hodgkin lymphoma, Mycoplasma infection and HIV infection have been implicated(1,2,8). It is suggested that vasculotropic organisms may elicit an inflammatory response and lead to PACNS(8). The presence of granulomata and absence of antibodies or immune complexes in the vessel wall suggest a disorder of cell-mediated immunity (CMI)(1). Other necrotizing vasculitis affecting the CNS should be ruled out by doing an erythrocyte sedimentation rate, rheumatoid factor and anti-nuclear antibodies(1,4). All these were negative in our patient. CSF analysis may show elevated proteins (<500 mg/dl) and lymphocytic pleocytosis (total cell count <200 cells/cu mm)(4,9). CSF studies are necessary to rule out infections and malignant conditions simulating PACNS. Serial CSF studies show close correlation with the disease(4,6). The EEG is sensitive (81% sensitivity) but lacks specificity(6). Diffuse or rarely focal slow wave pattern may be seen and can occur in other infectious or metabolic disorders involving the CNS(4). The CT scan may show an ischemic infarct, evidence of mass lesion, or may be completely normal(4). Gyral enhancement (suggesting breakdown of the blood-brain barrier) is also a non-specific finding(4). MRI may be more sensitive than the CT scan in identification of infarcts or edema(3). The initial diagnostic procedure is cerebral angiography showing the characteristic ‘sausage’ or ‘string of beads’ pattern, as seen in our patient(4). This is due to alternate focal stenosis and ectasia of the vessels(1,4,8,9). Segmental narrowing of cerebral vessels initially results from reversible inflammation and vasospasm but may be aggravated later due to scarring(3,9). The pattern is generally diffuse (rarely localized showing a mass effect) and can involve vessel of any caliber(1,2,8). Less specific findings are of microaneurysms, vague luminal narrowing or irregularity, hemorrhage or vessel disappearance(4). Similar angiographic findings are seen due to atherosclerosis, infections, emboli, neoplasia and drug abuse(1,4). The angiogram may be normal in biopsy proven cases of PACNS. This may be due to the disease involving vessles too small to be seen(1,4). Histological confirmation allows specific diagnosis. The sensitivity of biopsy (71%) is comparable to that of angiography(4). The presence of ‘skip-lesions’ decreases the yield of biopsy(1,4). Vasculitis is occassionally demonstrated at post-mortem examination(4). Any vessel of the brain or the spinal cord may be involved, with predilection for smaller leptomeningeal vessels. Arteries as well as veins show changes mainly in the media and adventitia(4,8). Transmural inflammation (infiltrate composed of multinucleated giant cells, lymphocytes, monocytes, histiocytes and plasma cells) with or without fibrinoid necrosis and perivascular inflammation is seen(1,2,8,9). Moore et al(1) has suggested the following criteria for establishing an antemortem diagnosis of PACNS: (i) Clinical pattern of headaches and multifocal neurological deficits present for at least 6 months, unless the deficits are severe at the onset or rapidly progressive; (ii) Cerebral angiography demonstrating segmental arterial narrowing; (iii) Exclusion of systemic inflammation or infection; (iv) Leptomeningeal or brain parenchymal biopsy demonstrating vascular inflammation or exclusion of alternate diagnosis. Our patient satisfied the first three criteria. A leptomeningeal or brain parenchymal biopsy was not done. An antemortem biopsy has not been possible in many of the previously reported cases(2,8-10). Calabrease, et al(4) have suggested that leptomeningeal and cortical biopsy be done with a normal or non-diagnostic angiogram and when the diagnostic likelihood is high. Alrawi, et al(11) suggest that a brain biopsy should be done since clinical indicators and angiography are not useful predictors of PACNS. Untreated cases carry a high mortality. Treatment with corticosteroids and cytotoxic agents (cyclophosphamide) has better outcome as compared to corticosteroids alone(1,4). Combination therapy should be initiated in patients with severe or rapidly progressive PACNS(4). Cyclophosphamide can be used in patients with mild stable diseases, which does not respond to corticosteroid therapy(4,5,7). The duration of therapy should be till the patient is symptom-free for one year(1,9). The angiogram is then repeated and treatment with cyclophosphamide rapidly tapered if the angiogram shows improvement or absence of additional abnormalities(1,3). Prednisolone is subsequently tapered slowly over 3-6 months if the patient remains well(1). Azathioprine has also been used in combination with steroids(6). It has been suggested that PACNS is clinically more heterogeneous than previously appreciated and may include relatively benign subsets(12). Survival in untreated cases is usually 1-3 yrs but some patients may have recurrent disease for over 4-5 yrs(1,2,8). Acknowledgment The authors thank Dr. Nilima A. Kshirsagar, Dean, Seth G.S. Medical College and KEM Hospital, Mumbai for permission to publish this article. Contributors: MPK and MST collected the clinical and laboratory data, performed the literature search, drafted the paper and will act as the guarantors for the paper. JRK and RKV contributed to the plan of investigations, interpretation of the collected data and revised the manuscript. Funding: None. Competing interests: None stated.
| ||
| References | ||
|
![]()