|
|
|
Original Articles Indian Pediatrics 2002; 633:639 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Long-acting GnRH Analogue Triptorelin Therapy in Central Isosexual Precocious Puberty |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Key words: GnRH analogue, Precocious puberty, Triptorelin. TRETAMENT with
progesterone Subjects and Methods CIPP was defined as the onset of puberty at an age less than 8 years in girls and 9.5 years in boys with pubertal baseline or GnRH stimulated LH and LH: FSH levels. Height was measured using a stadiometer. Orchidometer was used to measure the testicular volume and Tanner staging was done for pubertal assessment(13). Bone age (BA) was estimated by the TW2 method(14). Average tables of Bayley-Pinneau were used for estimating projected height (PH) as proposed by Kauli et al(15,16). Target height (TH) was calculated using the mid-parental height based on standard formula(17). Patients were treated with GnRH analogue triptorelin at a dose of 3.75 mg depot administered deep intramuscularly every 28 days. They were followed-up monthly for height, pubertal staging and complications. Pubertal suppression was evaluated 6 - monthly by GnRH stimulation test performed 2 days prior to the due dose of triptorelin(18). Estimation of BA and ultrasound pelvis were performed annually. Treatment was discontinued at the age of 10 years in girls and 12 years in boys. PH at the end of treatment was calculated using the tables of Bayley-Pinneau(15). Patients were considered to have attained final height when they had achieved a BA of 15 years and had a height gain of less than 0.5 cm in the preceding year(19). The mean, median and standard deviation values were determined for various parameters. Paired t-test was used for comparing pre and post treatment variables while unpaired t-test was used for comparing variables across two groups; P value less than 0.05 was considered significant. Correlation analysis was performed for determining the factors influencing outcome of final height and height gain. Results Thirty-five patients (30 girls and 5 boys) were included in the study. Boys had an earlier age at onset, greater height advancement in the form of higher heightSD and height compromise (difference of TH and PH) than girls (Table I). Both groups had advanced skeletal maturity as demonstrated by increased difference between chronological (CA) and BA (Table I). PH was below TH in 34.5% girls. Girls younger than 6 year at the time of treatment (n = 9) had greater heightSD, heightSDBA, difference between BA and CA and height compromise than those treated after the age of 6 year (Table I). A significantly greater number of these girls (1 out of 9) had PH lower than TH range than those treated at an older age (2 out of 21). Table I- Baseline Data and Treatment Details
* P < 0.05 for girls < 6 years and > 6 years ** P < 0.05 for boys and girls
Treatment details are summarized in Table I. All patients received treatment regularly. Treatment was started at an early age in boys than girls ( p = 0.04). Treatment resulted in regression of features of precocious puberty and secondary sexual characteristics in all the patients. During the course of treatment growth spurt was halted as demonstrated by a decrease in heightSD. Skeletal advancement decreased to a greater extent with decline in difference between BA and CA and in heightSDBA (Table II). Girls receiving treatment before the age of 6 years had a greater decline in heightSD, difference between BA and CA and heightSDBA than those treated at a later age (Table II). Table II__Outcome Measures
* P < 0.05 for girls < 6 years and > 6 years ** P < 0.05 for boys and girls
PH at the end of treatment was significantly higher than that at the start of treatment (p < 0.001 in both groups, Table I). Final height was lower than PH at the end of treatment by 1 ± 0.2 cm in girls and 0.2 ± 0.1 cm in boys. Height gain (6.4 ± 2.4 cm in girls and 7.6 ± 1 cm in boys) was similar in both groups (Table II). All subjects achieved final height in the TH range. Girls treated before the age of 6 years had greater height gain and similar final height than those treated at a later age. Height gain decreased with increasing age at treatment and girls treated after the age of 8 years gained only 4.7 cm.
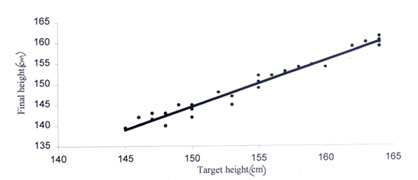
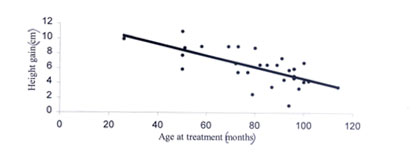
Correlation analysis of final height in girls revealed correlation with TH ( r = 0.979, Fig.1) and PH at the initiation of treatment ( r = 0.957). Height gain in girls was correlated with the age at treatment ( r = 0.715, Fig.2), duration of treatment ( r = 0.711), heightSDBA (r = 0.566) and difference between BA and CA at onset (r = 0.734). No side effects of GnRH analogue therapy were observed. Ultrasound of pelvis after discontinuation of therapy did not reveal evidence of polycystic disease in any girl. Girls attained menarche 1.2 ± 0.5 years after interruption of therapy. Discussion The height gain of 6.4 ± 2.4 cm in girls in this study is similar to that reported in recent studies(5,20). This is greater than earlier studies where it ranged from 2.4 - 4.8 cm (4, 5, 21). These studies had used the advanced tables of Bayley-Pinneau for predicting height at the onset while average tables were used in the current study. This could have overestimated PH at the initiation of treatment in these studies and thereby lowered height gain. We used average tables for height prediction as recommended by Kauli, et al(16). Attainment of final height in the TH range by all the subjects emphasizes the efficacy of GnRH analogue treatment in improving height outcome of these girls. Treatment with GnRH analogue therapy has been shown to regress the features of precocity preceded by a period of increase in growth rate and bone age enhancement. This was reflected in this study by the observation that increase in PH was observed only in the second year of treatment. Restoration of features of precocious puberty and menarche after a period of 1.2 ± 0.5 year following interruption of GnRH analogue therapy is similar to other studies(22). Efficacy of GnRH analogues in girls treated at an older age is not established. Reports suggesting no improvement, mild improvement and effects similar to younger girls have been reported(6,9). In this study girls treated after the age of 6 years had lower height gain than those treated earlier. This difference was greater in girls treated after the age of 8 years. These girls had lower bone age advancement and height compromise than those treated earlier. This indicates that these girls are milder variants of CIPP and may not benefit with GnRH therapy. This has been demonstrated in studies of GnRH therapy on girls older than 7.5 years where no significant height gain was obtained(10). Factors correlating with height gain include early age at treatment, greater difference between BA and CA at the initiation of treatment, greater decline in this difference during the course of treatment, longer duration of treatment and lower bone age at the end of treatment(23, 24). In our study girls treated at an early age and for a longer duration, with greater difference between BA and CA at the onset with lower difference at the end of treatment had the greatest height gain. Efficacy of GnRH analogue therapy in boys is not clearly established. Earlier studies indicated that GnRH analogue therapy does not improve the auxological outcome in boys(7,25, 26). These studies had limitations of treatment with drugs like cyproterone acetate and short acting GnRH analogue before triptorelin and presence of diseases like neurofibromatosis that may compromise height potential of these subjects(7). Recent studies indicate that GnRH therapy is beneficial in boys, a fact that is reiterated in this study(27). Correlation analyses for factors influencing outcome were not performed in boys due to the small sample size, no significant difference regarding age at treatment and BA advancement were however observed. Contributors: AB, JS, MK and PSNM were involved in patient management. AB planned the study, collected data, performed literature review and drafted the manuscript. MK and JS were involved in planning the study and drafting the manuscript. AKG was involved in bone age estimation and height projection. PSNM designed the study and critically reviewed the manuscript and will act as the guarantor. Funding: None Competing interests: None stated
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
REFERENCES | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()