|
|
Original Articles Indian Pediatrics 2002; 39:625-631 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Hepatitis B Vaccination in Premature and Low Birth Weight (LBW) Babies |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Ashish Bavdekar, Anand Pandit
Manuscript received:
December 24, 2001, Initial review completed: February 12, 2002, To assess the immune response of preterm and low birth weight babies (LBW) to hepatitis B (HB) vaccine. Setting: Neonatal Intensive Care Unit (NICU), postnatal ward and follow up clinics of KEM Hospital, Pune. Design: Open trial. Methods: 100 babies were enrolled in four study groups. Group I - preterm, gestational age (GA) < 34 weeks; Group II - GA 34 to 36 weeks; Group III full term <2.5 kg (LBW babies); and Group IV full term >2.5 kg (controls). A recombinant DNA HB vaccine was given at 0, 1, 2 and 12 month schedule. The first injection was administered as soon as the neonate was stabilized. Immune response in terms of anti HBs titres (AUSAB EIA Diagnostic kit) was measured one month after each of the first three injections and at the time of one year booster. Adverse events were monitored. Results: 88 and 62 babies completed the study till the third dose and one year booster dose respectively. Immune response of HB vaccine was uniformly good in all the study groups with 100% sero-conversion after the second dose itself. By one year (i.e. before the booster dose), very high titres were recorded in all 100%, with 85% demonstrating titres >1000 mIU/ml. Preterm and LBW babies had higher GMT as compared to full term babies till one month after third dose. By one year (before booster), full term babies had higher GMT than preterm and LBW babies. However, these differences were not statistically significant. The vaccine was well tolerated and safe and there were no adverse reactions. Conclusions: Immune response of preterm, LBW and full term babies to the new generation recombinant DNA HB vaccine was uniformly good. High and long term seroprotective levels were achieved after the second dose itself. Key words: Hepatitis B vaccine, Preterm immunization. IN 1991, the WHO Global
Advisory Group It is clear from many studies that for control of perinatal transmission, the first dose of HB vaccine must be given soon after birth preferably within 48 h(4). What still needs to be resolved is whether or not preterm and low birth weight (LBW) babies can be included in the policy of universal immunization starting at birth. The confusion has arisen chiefly because of conflicting reports of the immune response in preterms; and because the American Academy of Pediatrics (AAP) in 1994 revised its earlier recommendations and advised delaying the initiation of HB vaccine in preterms with a birth weight less than 2 kg till the age of 2 months(5). In India, more than 30% of newborns are less than 2.5 kg at birth, and many are less than 2 kg. Further, most of these babies have intrauterine growth retardation (IUGR) rather than true prematurity. Is this policy of delaying the first dose justified in our LBW babies, especially vis-a-vis the risk of confusing field workers? The aim of this study was to determine the immune response of preterm and LBW babies to a new generation, recombinant DNA, HB vaccine in comparison to full term neonates. Subjects and Methods The study was conducted in the Neonatal Intensive Care Unit (NICU) and postnatal wards of KEM Hospital, Pune. 100 neonates were enrolled in four study groups as seen in Table 1. {Group 1 = preterm, gestational age (GA) < 34 weeks; Group II = preterm, GA 34 to 36 weeks; Group III = full term < 2500 g IUGR babies, Group IV = full term, normal weight > 2500 g}. Parents were counseled and only those willing for all four injections and blood sampling were enrolled. Table I- Clinical Characteristics and Age at First Injection
Others include intraventricular hemorrhage, hypoglycemia, congenital heart disease, anemia, transient tachypnea and seizures. *Mean ± SD (range)
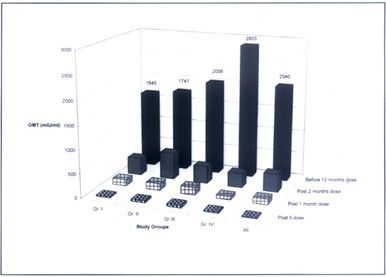
A new generation yeast derived recombinant DNA HB vaccine (Shanvac B, Shantha Biotechnics, Hyderabad) at a dose of 0.5 ml (10 mg) was given at 0, 1 month, 2 months and 12 months. All injections were given in the antero-lateral side of thigh. Medical Social Workers (MSW) encouraged compliance with counseling and home visits. The zero dose was given in the NICU or ward as soon as the baby was considered ‘stable’. The subsequent doses were given in follow up clinics. After each dose of the vaccine babies were monitored for any evidence of adverse reaction such as anaphylaxis, fever, local pain, erythema, tenderness, induration, vomiting etc. Adverse reactions were graded as 0-absent, 1-mild, 2-moderate, 3-severe. Monitoring for reaction was done by staff members of the NICU and ward after 0 dose. For subsequent doses, the baby was observed in the follow up clinics for half-hour after the injection for any immediate reactions like anaphylaxis. Further monitoring (for 48 h) was carried out by parents at home (parents were informed about the possibility of above mentioned side effects and advised to report, if any). The MSW made a phone call after 48 h to confirm the absence of side effects. Serum samples for antibody estimation were obtained one month after the first, second and third dose and just before the 12 months dose. All samples were taken by venepuncture in upper limb under all aseptic precautions. Anti-HBs titres were assessed quantitatively by microparticle enzyme immunoassay (AUSAB EIA kits, Abbott Laboratories). The laboratory personnel were blinded to the subjects’ identity. All the samples (four sets) were tested in two batches of kits. For internal (batch) validity, two samples (lab controls) were tested in both the batches. The result were stable. Levels of anti HBs > 10 mIU/ml were taken as evidence of seroprotection while levels > 100 mlU/ml were considered as evidence of long term seroprotection(6). Samples positive for anti HBs were included for calculation of geometric mean titre (GMT). Students ‘t’ test was used to compare anti HBs GMT between various groups. The study was approved by the Ethical Committee of our center. Free and informed written parental consent was obtained in all cases. Results Of the 100 enrolled babies, 88 completed the study upto one month after the third dose of vaccine, and 62 completed the entire study i.e., upto the end of 12 months (last dose). The reasons for the drop out in the first phase were: death (n = 4), transfer (n = 4), refusal (n = 2), lost to follow up (n = 2). The further drop outs were due to death (n = 5), transfer (n = 11), refusal (n = 4) and lost to follow up (n = 6). All deaths were related to complications of prematurity and LBW. Clinical parameters of the study subjects are seen in Table I. There were no demographic differences between babies who completed the study and those who did not. Associated illnesses or problems in the study groups are seen in Table I. Age of initiation of first dose of vaccine: The age at first dose of vaccination ranged from 4 - 30 days in the smallest weight group and 0 - 15 days in the full term normal weight group with a mean of 8.0 ± 7.8 days for the whole group. Side effects: There were no adverse reactions or side effects after any of the doses throughout the entire study. None of the deaths were related to vaccinations. Seroprotection: Seroprotection (i.e., anti HBs antibodies > 10 mIU/ml), at one month after the first dose were 67%, 57%, 70%, and 50% in groups I, II, III and IV respectively. Seroprotection was 100% in all groups 1 month after the second dose, and remained 100% after the third and before the last dose. Antibody titres had reached long term protective levels (>100 mIU/ml) in 54 of the 88 babies (61%) after the second dose, in 84 of the 88 babies (95%) by the end of third dose and in all 62 babies (100%) at one year. At one year, 85% subjects had achieved antibody titres > 1000 mIU/ml. Geometric mean titres (GMT): Serial GMT of anti HBs antibodies in different groups are seen in Fig.1. All the study groups showed modest increase of GMT after the second dose (post one month dose) itself. GMT rose further after the third dose reaching a mean of 452 mIU/ml in preterm (Group I and II) and 334 mIU/ml in full term babies (Group III and IV). LBW babies (Group I, II, III) had a higher GMT of 415 mIU/ml as compared to 304 mIU/ml in normal weight babies (Group IV); differences between various groups were not significant. At one year (before last dose), GMT showed more then 5 fold increase in antibody titres in all the 62 babies followed up. None of the babies showed decreasing titres. On the whole GMT at 1 year were higher in normal weight (Group IV - 2854 mIU/ml) control babies than the LBW (Group I, II and III - 1814 mIU/ml) babies (p = 0.08). Similarly GMT were higher in full term babies Group III and IV as compared to preterm Group I and II (2,357 mIU/ml in full term vs. 1,690 mIU/ml in preterms respectively) (p = 0.18). Discussion The main aim of this study was to evaluate the immune response of preterm and LBW babies to HB vaccine. We enrolled 100 babies with gestational ages ranging from 27 weeks to 40 weeks and with birth weights ranging from 1155 g to 3575 g. We used the schedule specifically recommended for high risk babies namely four doses at 0, 1, 2 and 12 months. Despite the high mortality rate in the small preterms and despite transfer of residence in many we achieved a high compliance rate with 88% and 62% completing the study upto the third and last dose respectively. The immune response to HB vaccine in our study was uniformly good in preterms, IUGR babies and normal weight neonates. The overall seroconversion rate was 100% with remarkably high titres reaching well above 1000 mIU/ml in 85% by the one year booster dose (mean GMT of whole group 2040 mIU/ml). In other studies using HB Vax(7) and Engerix B(8), the final GMTs did not cross 500 mIU/ml and 750 mIU/ml respectively. The very high and ‘long term sero protective level’ achieved in our study are due to the very high immunogenecity of the vaccine used. Previous studies using this vaccine have also reported much higher titres and protective levels as compared to other recombinant DNA vaccines(9). The immune response was more than satisfactory in all the study groups with high GMT at all stages of testing. Preterm babies, infact, had higher GMT as compared to full term babies until one month after the third dose. By age one year and before the fourth dose, full term babies had higher GMT than preterms. The IUGR group too, showed good immunological response throughout the study. Though there are no reported studies from India, data from other countries (both developing and developed) regarding immune response in preterms is conflicting(10,11). Huang, et al,(9) Blondecham, et al(8) and others(12-14) have shown less than 90% seroprotection with low GMT in preterms at the end of their schedule, especially, in small preterms <1500 g. An interesting study in small preterms suggested better immune response if first dose was delayed till 30 days of age(15). Other studies have reported excellent response in preterm babies irrespective of birth weight or age of first injection(16). The varying results could well be due to differences in ethnicity, type of vaccine used and the timing of the first vaccination.
It has been suggested recently that the first dose of HB vaccine should be delayed to 6 to 8 weeks, the advantage being (a) possibility of combination with DPT (and also Hib vaccine), thereby reducing the number and cost of injection(18, 19) and (b) better immune response in preterms and babies with IUGR if initiation is delayed(15). However, it is important to remember that India is in the intermediate to high risk zone for HBV and perinatal transmission can be halted effectively only if vaccination commences within 48 h of birth(4,17). In our smallest preterm group with mean birthweight <1500 g, the first dose of vaccine was delayed in some as long as 30 days mainly because, as per protocol, the vaccine was given only after the baby was stable. These were NICU patients with serious clinical problems including sepsis and respiratory distress. In other babies, who were not so ill, the first dose was given as early as four days of life. We found no difference in the immune response in these babies. However, whether, ‘sick’ neonates can be given the vaccine within 48 hr of birth without waiting for ‘stabilization’ remains to be seen. If possible, it would be particularly advantageous as these are the high risk groups, receiving multiple transfusions, blood products and injections in the NICU. The 0, 1, 2 and 12 schedule used in our study was obviously very effective. All the babies (100%) seroconverted after the second dose itself (with more than 60% reaching ‘long term seroprotective levels’). This suggests that the third dose (at second month) is probably unnecessary even in preterms, LBWs and other high risk babies. Interestingly, in our study, antibody titres showed more than a five fold increase between the third and last dose, even though no further injections were given during this period. Obviously, once stimulated antibodies continue to increase with time; boosters accentuate the increase. The vaccine was well tolerated in all subjects and there were no adverse reactions. The safety of the vaccine in normal neonates and adults has been reported previously(9,16). Acknowledgement We thank our Medical Social Workers for diligently following up the babies. Contributors: ShB designed the study and drafted the paper and will act as guarantor. SnB and SC conducted the study. SN carried out the antibody testing. AB helped in analysis and interpretation of the data. AP and RP helped in designing the study and monitored the project. Funding: Shantha Biotechnics Pvt. Ltd., Hyderabad. Competing interests: RP is an employee of Shantha Biotechnics Pvt. Limited, a manufacturer of Hepatitis B vaccine.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()