|
|
|
Indian Pediatr 2021;58: 25-28 |
 |
Suctioning First or Drying First During
Delivery Room Resuscitation: A Randomized Controlled Trial
|
|
Ashok Kumar, 1
Ravi Prakash Yadav,1
Sriparna Basu1
and TB Singh2
From 1Neonatal Unit, Department of Pediatrics
and 2Biostatistics Unit, Institute of Medical
Sciences, Banaras Hindu University, Varanasi, UP, India.
Correspondence to: Dr Ashok Kumar, Department of
Pediatrics, Institute of Medical Sciences, Banaras Hindu
University,
Varanasi 221005, India.
Email:
[email protected]
Received: July 23, 2019;
Initial review: November 05, 2019;
Accepted: July 13, 2020.
Clinical Trial Registration: CTRI/2017/04/008340
|
|
Objective: To compare
the effect of suctioning first or drying first on the composite
outcome of hypothermia or respiratory distress in depressed
newborns requiring delivery room resuscitation.
Design: Open-label,
randomized, parallel-group, controlled trial.
Setting: Delivery
room and neonatal intensive care unit of a tertiary-care
teaching hospital.
Patients: Depressed
newborns (n=154) requiring initial steps of resuscitation
at birth.
Intervention: During
delivery room resuscitation eligible new-borns were randomly
allocated to receive either suctioning first or drying first (77
newborns in each group).
Main outcome measure:
Composite incidence of hypothermia at admission or respiratory
distress at 6 hours of age.
Results: Both groups
were comparable with regard to maternal and neonatal
characteristics. Composite outcome was similar in both the
groups [46 (59.7%) vs 55 (71.4%)] in suctioning first and
drying first, respectively [RR (95% CI), 0.84 (0.66–1.05); P=0.13].
Incidence of hypothermia, respiratory distress at admission and
oxygen saturation at 6 hours were also similar. On admission to
NICU, hypothermia was observed in 26 (33.8%) neonates in
suctioning first group and 33 (42.8%) neonates in drying first
group but by one hour of age the proportion of hypothermic
neonates was 13 (16.9%) and 14 (18.1%), respectively.
Conclusion: In
newborns depressed at birth, the sequence of performing
initial steps, whether suctioning first or drying first, had
comparable effect on composite outcome of hypothermia at
admission or respiratory distress at 6 hours of age.
Key words: Hypothermia, Initial
steps, Mortality, Newborn, Outcome, Respiratory distress.
|
A pproximately 10%
of newborns require some assistance to initiate and sustain
effective breathing at birth [1], and perinatal asphyxia
accounts for 23% of 4 million neonatal deaths each year
globally [2]. Skilled delivery room resuscitation can
prevent many of these deaths and neurodevelopmental
handicaps in survivors.
All depressed newborns requiring delivery
room resuscitation should receive ‘initial steps’ before
initiating positive pressure ventilation. These essentially
constitute temperature maintenance, positioning, suction-
ing, drying and tactile stimulation. Suctioning is done to
clear the airway and drying is done to prevent heat loss.
Though the sequence of suctioning followed by drying has
been endorsed as the part of initial steps in neonatal
resuscitation program (NRP) of the American Academy of
Pediatrics (AAP) [3], it is based on expert opinion rather
than evidence. It is not clear whether the same sequence
should be followed in a resource-limited settings of lower
and middle income countries, where the danger of hypothermia
constitutes a bigger threat [4-6]. Due to this dilemma, the
Indian NRP (first edition) [7], advocated for the sequence
of drying followed by suctioning as initial steps in Indian
scenario. However, in neonatal resuscitation module of
Facility-based newborn care [8], the sequence has been
changed to suctioning first, followed by drying.
Contradictory recommendations have led to confusion among
health professionals, with variations in practice and
training. The objective of the present study was to compare
the effect of suctioning versus drying as a first procedure
during delivery room resuscitation on the composite outcome
of hypothermia at admission or respiratory distress at 6
hours of age.
METHODS
This open-label, randomized controlled
trial was conducted in the delivery room and neonatal
intensive care unit (NICU) of a tertiary care teaching
hospital of central India from March, 2016 to August, 2017.
The study protocol was approved by the Institutional Ethics
Committee. Written informed consent was obtained from the
parents before delivery. The cases was excluded, if there
was insufficient time to obtain informed consent.
Consecutively delivered inborn neonates
who were depressed at birth and required initial steps of
resuscitation were included. Depression at birth was defined
as presence of apnea or gasping and/or limp or poor muscle
tone. Neonates delivered through meconium stained liquor,
major congenital anomalies and cases where there was
insufficient time to obtain consent were excluded. Antenatal
details of the mothers including maternal age, gravida,
parity, receipt of antenatal care, complications of
pregnancy, evidence of fatal distress, mode of delivery, and
relevant investigations done in the pregnant mother,
including ultrasonography were noted.
Eligible newborns were randomized into
one of two groups (suctioning first or drying first) using
random permuted blocks of 4, 6 or 8. The randomization
sequence was prepared by an independent person not involved
in the conduct of study. Allocation of newborns to different
groups was done using serially numbered, opaque and sealed
envelopes.
All deliveries were attended by two
pediatric residents who were trained in neonatal
resuscitation as per AAP guidelines. After delivery, if a
newborn was found to be apneic or limp, the umbilical cord
was clamped immediately and baby was placed under radiant
warmer with neck slightly extended. By this time, one member
of the team or a staff nurse opened the sealed envelope and
further sequence of initial steps was performed as per
randomization. During resuscitation, oxygen saturation was
recorded from right hand or wrist, using hand-held Masimo
pulse oximeter. For suctioning, wall mounted suction was
used with a pressure not exceeding 100 mm of Hg. Each
attempt at suctioning was limited to no more than 3 to 5
seconds, and care was taken to avoid vigorous or deep
suctioning. We used a pre-warmed towel to dry the baby and
removed wet towel to prevent further heat loss. After
completing initial steps including tactile stimulation, if
the baby continued to have apnea/gasping breathing or
bradycardia (heart rate 100/minute), positive pressure
ventilation was initiated. The remaining steps of
resuscitation were similar in the two groups.
All neonates were admitted to NICU and
were monitored and managed as per unit protocol. Babies were
kept under radiant warmer with temperature set at 36.5 oC.
Babies were monitored using a predesigned proforma for heart
rate, oxygen saturation, temperature, capillary refill time,
respiratory rate, and other signs of respiratory distress
(chest wall retractions, grunting and bilateral air entry
into the chest). Investigations included blood glucose,
serum electrolytes, chest X-ray, sepsis workup (complete
blood count, absolute neutrophil count, C-reactive protein
and blood culture), if needed, arterial blood gas analysis
and renal function tests. Other tests included
echocardiography and cranial ultrasonography, as and when
necessary. Respiratory support was given via oxygen hood,
continuous positive airway pressure (CPAP), high flow nasal
cannula (HFNC) or mechanical ventilation as per need.
Intravenous fluids, parenteral nutrition, and feeding were
provided. Complications were managed as per our unit
protocol.
Primary outcome variable was composite
outcome of admission hypothermia or respiratory distress at
6 hours of age. Hypothermia was defined as rectal
temperature <36.5oC.
Rectal temperature was recorded using a low-reading rectal
thermometer. Respiratory distress was defined as presence of
at least one of the following: respiratory rate >60/minute,
chest wall retractions and grunting. Secondary outcome
variables included the need and duration of positive
pressure ventilation, chest compressions and medication use
during delivery room resuscitation, oxygen saturations
during first 10 minutes of age, incidence of hypothermia and
respiratory distress within 24 hours, development of
complications and duration of hospital stay and outcome.
Assuming an expected incidence of the
need for delivery room resuscitation of 10% [3], a precision
(d) of 0.05 and level of confidence of 95%, the sample size
calculated was 138. Considering 10 % attrition rate, the
total sample size was 154 newborns, 77 in each group
(www.kck.usm.my/ppsg/statistical_resources/SSCPS
version1001.xls).
Statistical analyses: The
statistical program SPSS version 16.0 was used for analysis.
Independent samples t test/Mann Whitney U test and Fisher
exact test were used as applicable to compare parametric and
non-parametric variables. Risk ratios (RR) with 95% CI were
calculated for outcome variables. The data were analyzed on
intention to treat basis. A P value of <0.05 was
considered statistically significant.
RESULTS
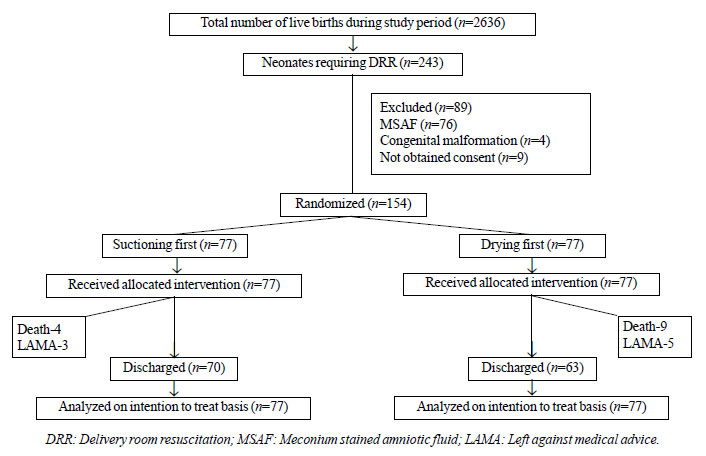
Each group included 77 neonates, and all
neonates received their allocated intervention (Fig.
1). Both the groups were similar with respect to
maternal and neonatal characteristics, except the incidence
of eclampsia, which was significantly higher in suctioning
first group (Table I).
 |
|
Fig.1 Flow of
participants in the study.
|
Table I Maternal and Neonatal Characteristics of Study Participants
|
Suctioning first
|
Drying first
|
|
(n=77) |
(n=77) |
|
Maternal characteristics |
|
|
|
*Maternal age, y |
26.2 (4.5) |
25.9 (4.1) |
|
#Gravida |
2 (1 -3) |
2 (1 -3) |
|
PIH/ Pre-eclampsia |
7 (9) |
6 (7.7) |
|
Eclampsia |
21(27.2) |
10 (12.9) |
|
Antepartum hemorrhage |
4 (5.1) |
5 (6.4) |
|
PV leak >18 h |
11 (14.2) |
16 (20.7) |
|
Maternal fever |
2 (2.6) |
2 (2.6) |
|
Fetal distress |
10 (12.9) |
15 (19.4) |
|
Cesarean section |
56 (72.8) |
53 (68.9) |
|
Neonatal characteristics |
|
|
|
*Gestation, wk |
35.4 (3.5) |
34.7 (3.1) |
|
*Birthweight,
g |
2123 (67) |
2131 (64) |
|
Male gender |
43 (55.8) |
46 (59.7) |
|
#APGAR score |
|
|
|
1 min |
4 (3-5) |
4 (3-6) |
|
5 min |
7 (6-8) |
8 (7-9) |
|
Values in no. (%) except*mean (SD) or #median
(IQR); PIH: Pregnancy induced hypertension; PV: Per
vaginal; P>0.05 for all variables between the two
groups. |
The composite outcome of hypothermia at
admission or respiratory distress at 6 hours of age was
similar in suctioning first and drying first, respectively
[46 (59.7%) vs. 55 (71.4%); RR (95% CI), 0.84 (0.66-1.05);
P = 0.13] (Table II). Among the secondary
outcome variables, oxygen saturation within 10 minutes after
birth, incidence of hypothermia at admission, and
respiratory distress at different time intervals during
first 6 hours of age were also similar (P>0.05) (Table
II). On admission to NICU, 26 (33.8%) neonates in
suctioning first group and 33 (42.8%) neonates in drying
first group experienced hypothermia (Table II).
By one hour of age hypothermia was observed in 13 (16.9%)
and 14(18.1%) neonates, respectively. The differences were
not significant.
Table II Outcome Variables in Neonates in the Two Study Groups
|
Variable |
Suctioning first (n =77) |
Drying first (n=77) |
Relative risk (95% CI) |
|
Composite outcome, n (%) |
46 (59.7) |
55 (71.4) |
0.84 (0.66-1.05) |
|
Hypothermia at admission |
26 (33.8) |
33 (42.8) |
0.79 (0.52-1.18) |
|
Respiratory distress at 6 h |
34 (44.2) |
38 (49.4) |
0.89 (0.64-1.25) |
|
Oxygen saturation (%)a |
|
|
|
|
At 1 min |
60 (56-63) |
59 (54-63) |
- |
|
At 2 min |
68 (64-72) |
68 (64-72) |
- |
|
At 5 min |
84 (82-87) |
84 (81-86) |
- |
|
At 10 min |
94 (92-95) |
93 (92-95) |
- |
|
Bag and mask ventilation |
73 (94.8) |
75 (97.4) |
0.97 (0.91-1.04) |
|
Duration, sa |
30 (30-30) |
30 (30-60) |
- |
|
Bag and tube ventilation |
50 (64.9) |
43 (55.8) |
1.16 (0.89-1.50) |
|
Duration, mina |
5 (5-10) |
5 (1-10) |
- |
|
Chest compressions
|
0 |
4 (5.1) |
0.11 (0.01-2.03) |
|
Adrenaline usage |
0 |
2 (2.5) |
0.20 (0.01-4.10) |
|
Death |
4 (5.2) |
9 (11.7) |
0.44 (0.14-1.38) |
|
All values in no (%) except amedian (IQR); RR:
Relative risk; Composite outcome - hypothermia at
admission or respiratory distress at 6h of age;
P>0.05 for all variables between the two groups. |
Resuscitation details for both the groups
are summarized in Table II. No significant
difference was observed in the extent of delivery room
resuscitation received by both the groups. Four (5.2%)
neonates expired in the suctioning first group, whereas 9
(11.7%) expired in the drying first group (P>0.05) (Table
II).
DISCUSSION
The present study demonstrated that
suctioning first or drying first during initial steps of
delivery room resuscitation result in comparable rates of
composite outcome of hypothermia at NICU admission or
respiratory distress at 6 hours of age in depressed
newborns. We could not find any study in literature which
investigated the comparative efficacy of drying versus
suctioning as a first intervention during delivery room
resuscitation.
The incidence of hypothermia was quite
high in our study cohort, as compared to previous data from
India [9-11]. Although newborns were resuscitated under
radiant warmer, they were transported to NICU without any
additional source of heat, which might have led to higher
incidence of admission hypothermia in our study population.
Preponderance of preterm newborns in study population might
have added to the burden of hypo-thermia in study cohort. We
did not measure the temperature of newborns in delivery
room before transporting them to NICU. The possibility that
some babies developed hypothermia during resuscitation
cannot be excluded. It is well known that hypothermia at
admission is associated with poor outcome [4-6]. We did not
use polyethylene wraps to maintain temperature of extremely
preterm newborns at birth, which obviates the need for
drying in these cases, as drying was applied as one of the
comparator interventions in the present study.
We observed no difference in the extent
and duration of resuscitative interventions between the two
groups. The mortality rates were also comparable in the two
groups.
To conclude, it makes little difference
to the outcome whether newborns are suctioned first or dried
first and either approach is acceptable. However, to bring
uniformity and consistency among health professionals and
to avoid confusion in the implementation of NRP guidelines,
we should follow an approach which is in agreement with
standard guidelines unless there is a definite evidence of
preferring one approach over the other.
Contributors: AK, SB: conceptualized
and designed the study, coordinated and supervised data
collection, drafted the initial manuscript, and reviewed and
revised the manuscript; RPY: designed the data collection
instruments, collected data, carried out the initial
analyses, and reviewed and revised the manuscript; TBS:
analyzed the data, and reviewed and revised the manuscript.
All authors approved the final manuscript as submitted and
agree to be accountable for all aspects of the work.
Ethical clearance:
Institutional Ethics Committee of Institute of Medical
Sciences, BHU; No. Dean/2014-15/EC/1455 dated 17 October,
2015.
Funding: None; Competing interests:
None stated.
|
WHAT IS ALREADY KNOWN?
•
During delivery room
resuscitation, the sequence of performing suctioning
and drying is based on expert opinion rather than
any evidence.
WHAT THIS STUDY ADDS?
•
Suctioning first or drying first during delivery
room resuscitation has comparable effect on the
composite outcome of admission hypothermia or
respiratory distress at 6 hours of age in newborn
infants.
|
REFERENCES
1. Barber CA, Wyckoff MH. Use and
efficacy of endotracheal versus intravenous epinephrine
during neonatal cardiopul-monary resuscitation in the
delivery room. Pediatrics. 2006;118:1028-34.
2. Black RE, Cousens S, Johnson HL, et
al; Child Health Epidemiology Reference Group of WHO and
UNICEF. Global, regional, and national causes of child
mortality in 2008: A systematic analysis.
Lancet. 2010;375:1969-87.
3. Wyckoff MH, Aziz K, Escobedo MB, et
al. Part 13: neonatal resuscitation: 2015 American Heart
Association Guidelines Update for Cardiopulmonary
Resuscitation and Emergency Cardiovascular Care. Circulation.2015;132:
S543-60.
4. Sodemann M, Nielsen J, Veirum J,
Jakobsen MS, Biai S, Aaby P. Hypothermia of newborns is
associated with excess mortality in the first 2 months of
life in Guinea-Bissau, West Africa. Trop Med Int Health.
2008;13:980-6.
5. Miller SS, Lee HC, Gould JB.
Hypothermia in very low birth weight infants: Distribution,
risk factors and outcomes. J Perinatol. 2011;31:S49-56.
6. Mullany LC, Katz J, Khatry SK, LeClerq
SC, Darmstadt GL, Tielsch JM. Risk of mortality associated
with neonatal hypothermia in southern Nepal. Arch Pediatr
Adolesc Med. 2010;164:650-6.
7. Neonatal Resuscitation: India. 1st ed.
National Neonato-logy Forum of India; 2013.p.5.
8. Neonatal Resuscitation Module.
Facility Based Newborn Care: Ministry of Health and Family
Welfare, Government of India, New Delhi;2014. p.9-16.
9. Kumar R, Aggarwal AK. Body
temperatures of home deli-vered newborns in north India.
Trop Doct. 1998; 28: 134-6
10. Kaushik SL, Grover N, Parmar VR,
Kaushik R, Gupta AK. Hypothermia in newborns at Shimla.
Indian Pediatr. 1998; 35: 652-6.
11. Bang AT, Reddy HM, Deshmukh MD, Baitule SB, Bang RA.
Neonatal and infant mortality in the ten years (1993 to
2003) of the Gadchiroli field trial: effect of home-based
neonatal care. J Perinatol. 2005; 25(Suppl 1): S92-107.
|
|
|
 |
|
