|
|
|
Indian Pediatr 2019;56:60-62 |
 |
ILAE Classification of
Seizures and Epilepsies: An Update for the Pediatrician
|
|
R Dhinakaran and Devendra Mishra
From Department of Pediatrics, Maulana Azad Medical College
(University of Delhi) and associated Lok Nayak Hospital, New Delhi,
India.
Correspondence to: Dr Devendra Mishra, Department of Pediatrics,
Maulana Azad Medical College, Delhi 110 002, India. Email:
[email protected]
|
|
The International League Against Epilepsy (ILAE) recently published an
updated classification of seizures and epilepsy. This updated
classification aims to have a better organized classification and ensure
better understanding of terms, in addition to including new seizure
types. As both seizures and epilepsy are important childhood conditions,
we herein list some of the important aspects of the updated
classification for the benefit of the general pediatricians. The full
classifications are available at the ILAE website.
Keywords: Diagnosis,
Epilepsy, Guidelines, International league against epilepsy, Management.
|
|
S
eizures are a common pediatric problem, and of
considerable interest to pediatricians [1,2]. Classification of seizures
and epilepsy is the cornerstone in the evaluation and management of
seizures. It helps in understanding the types of seizure, identifying
and labeling the type of epilepsy, and grouping similar entities into
specific syndromes – thereby guiding antiepileptic therapy and patient
counseling. Epilepsy classification is primarily used for the diagnosis
of patients, but it is also critical for research, communication among
clinicians and researchers, and development of antiepileptic therapies
[3].
The International League Against Epilepsy (ILAE) has
been playing a pivotal role in classification of epilepsy [4-7]. The
1981 and 1989 ILAE classifications were a major breakthrough in
understanding the types and classification of seizures and epilepsy
[4,5]. Since then, multiple modifications and revisions have been
proposed [6,7]. In 2017, ILAE published an updated classifications of
both seizures [8] and epilepsies [3]; these being the "first new
official papers on classification from the ILAE since 1989" [9]. With
advancement in technology and research, new insight has been gained in
understanding the phenotypic pattern and the basic mechanism of seizure,
thus making revision a necessary process. The stated purpose of
revisions is to include new seizure types, have a better organized
classification and to enable usage of appropriate terms for better
understanding [3].
We herein list some of the important aspects of the
revised classification for the benefit of the readers – these include,
among others, new focal seizure types which were earlier in generalized
category alone (e.g., epileptic spasm could be focal as well as
generalized), new generalized types (like myoclonic atonic and epileptic
spasm), and classifying focal seizure by its "first clinical
manifestation" [8]. The full documents are available at the ILAE website
(https://www.ilae.org/guidelines/definition-and-classification).
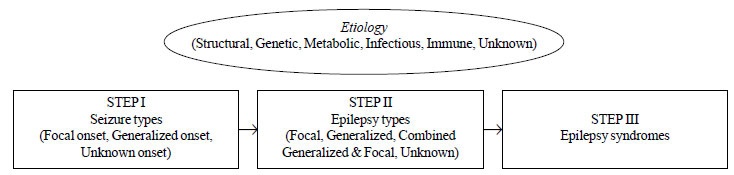
The new classification framework of epilepsy is a
multilevel classification with four main components; three of them
sequential viz., (i) the seizure type, followed by (ii)
the epilepsy type, and then (iii) the epilepsy syndrome. The
fourth component, identifying etiology, is an overarching activity,
continuing at each individual step (Fig. 1). The framework
is designed to enable classification of epilepsy in different clinical
settings implying that patient characterization will be possible at
every level, depending on the resources available to the clinician
making the diagnosis [3]. Supporting information viz., Video
record, Electro-encephalography (EEG), neuroimaging, gene mutations and
autoimmune panel, if available, are to be utilized in classifying
epilepsy type and/or epilepsy syndrome [3].
 |
|
Fig. 1 Schematic representation of
the multi-level classification of seizure and epilepsy (ILAE,
2017).
|
Classifying Seizures
The new basic 2017 classification of seizure is based
on three key features viz., (i) locus of seizure origin in
brain; (ii) level of awareness during seizure; and, (iii)
other features. The basic operational seizure type classification
includes [8]: Focal onset seizures (Aware/Impaired awareness;
Motor/Non-motor onset; and Focal to bilateral tonic-clonic); Generalized
onset (Motor/Non-motor (Absence)); and Unknown onset (Motor/Non-motor;
Unclassified).
Inclusion of new seizure types: The new seizure
types included in the classification are enlisted in Box 1.
|
BOX I Newer Terminologies for Seizure
Type in ILAE Seizure Classification, 2017
Focal seizures
Motor: Epileptic spasms, myoclonic, tonic,
tonic clonic, clonic, atonic, hyper-kinetic, automatism
Non-motor: Behavior arrest, emotional
Focal to bilateral tonic-clonic
Generalized seizures
Absence with eyelid myoclonia, epileptic
spasms, myoclonic–atonic, and myoclonic–tonic–clonic
|
Clarification of impairment of consciousness:
Consciousness is a complex phenomenon with both subjective and objective
components. In the 2017 classification, awareness has been chosen to be
the best surrogate marker of consciousness, and is simpler to evaluate
[8]. Awareness is operationally defined as "knowledge of self and
environment" [8].
Re-classification of certain seizure types into
either focal or generalized onset: Seizures are classified by
earliest prominent motor or non-motor features; even though, uncertainty
is present in every seizure classification [8]. The term ‘bilateral’ is
used for propagation patterns and ‘generalized’ for seizures that engage
bilateral networks from onset. Few seizure types like epileptic spasms,
myoclonic, tonic, tonic-clonic, clonic, atonic, which were previously
included only in generalized-onset seizures are now also included in
focal-onset seizures [8].
Classification of seizure of unknown onset:
Situations in which patient is alone or asleep or the attender is not
able to describe the seizure onset clearly is classified as Seizure of
unknown onset. If clinician is confident that an event is seizure but
cannot classify it due to incomplete information, it is grouped under
unclassified seizures. In the 2017 classification, Seizure of unknown
onset is further classified as tonic-clonic, epileptic spasms or
behavior arrest depending upon the predominant motor or non-motor
activity noticed during the episode [8]. This is essential in guiding
treatment, and for reclassification into focal or generalized onset with
future episodes. In this regard, the term ‘unknown onset’ is a
placeholder – not a characteristic of the seizure [8].
New terms for old ones: Some of the terms used in
seizure-classification lack community acceptance or public
understanding. The terms dyscognitive, simple partial, complex partial,
psychic, and secondarily generalized were eliminated. The term ‘partial’
was replaced by ‘focal’, as the term partial conveys a sense of part of
a seizure, rather than a location or anatomic system. ‘Focal to
bilateral tonic-clonic’ replaced ‘focal seizure with secondary
generalization,’ as this term can better reflect the propagation pattern
of a seizure (Table I) [8].
TABLE I New Terms Introduced in the ILAE Seizure Classification, 2017
|
Old terms
|
New terms |
|
Partial |
Focal |
|
Simple partial |
Focal aware |
|
Complex partial |
Focal impaired awareness |
|
Psychic |
Cognitive |
|
Secondary generalized
|
Focal to bilateral tonic-clonic |
|
tonic- clonic |
|
|
Arrest, Freeze, Pause,
|
Behavior arrest |
|
Interruption |
|
|
Dyscognitive |
Focal impaired awareness |
|
Astatic |
(Focal or generalized)atonic |
|
Grand mal |
Generalized tonic clonic,Focal to bilateral tonic clonic,
Unknown onset tonic clonic |
|
Infantile spasm |
Epileptic spasm |
|
Psychomotor |
Focal impaired awareness |
Updated glossary of seizure terms: Glossary of
seizure terms has also been updated and it includes new definition for
terms like emotional seizure, eyelid myoclonia, myoclonic atonic,
behavior arrest, unaware, and unclassified seizure [10]. Common
descriptors used to describe seizures have also been standardized in the
new 2017 classification [10].
Classifying Epilepsy Types
A new group of combined generalized and focal
epilepsy has been introduced in the epilepsy type. Idiopathic
generalized epilepsy was renamed as Genetic generalized epilepsy, which
includes Childhood absence epilepsy, juvenile absence epilepsy, Juvenile
myoclonic epilepsy and Generalized tonic–clonic seizures alone [3]. The
terms ‘Epileptic encephalopathy’ and ‘Developmental encephalopathy’ have
been redefined, and ‘malignant’ and ‘catastrophic’ are omitted. The term
‘benign’ used in some epilepsy syndromes like BECTS (Benign epilepsy
with centro-temporal spikes) is now replaced by ‘self-limited’ or ‘pharmaco-responsive’
depending on the situations [3].
Epilepsy Syndromes
Diagnosis of an Epilepsy syndrome, if possible, is
the third level of diagnosis [10]. An epilepsy syndrome is diagnosed on
the basis of all or some of age at presentation, seizure type, EEG
findings, etiological substrate, neuroimaging, genetic analyses,
occurring in a typical pattern [10]. Recognition of a syndrome helps in
determining etiology, evaluating for co-morbidity, deciding management,
and conveying prognosis.
Labeling Etiology
This epilepsy classification lays stress on
determining etiology at all stages along the diagnostic process,
starting from the initial presentation and evaluation. Six major
etiological categories have been recognized in the classification (Fig.
1), with an understanding that a patient’s epilepsy may be
classified into more than one etiological group. An example would be a
‘structural’ cause (cortical tuber) in a ‘genetic’ condition (tuberous
sclerosis).
Conclusions
These new classifications of seizures and the
epilepsies are likely to lead to improved understanding of seizure
etiology, making appropriate diagnosis and will guide targeted therapies
to the patient. This classification may also help in greater ease of
communication about seizure types among clinicians, the non-medical
community, and researchers. The simultaneously published instruction
manual on applying the seizure classification terminology will immensely
assist in everyday clinical practice [9]. A companion piece to present
these concepts for people with epilepsy and their caregivers is also
available [10].
Funding: None; Competing Interests:
None stated.
References
1. Mishra OP, Upadhyay A, Prasad R, Upadhyay SK,
Piplani SK. Behavioral problems in Indian children with epilepsy. Indian
Pediatr. 2017;54:116-20.
2. Sajjan S, Jain P, Sharma S, Seth A, Aneja S.
Injuries in children with epilepsy: A hospital-based study. Indian
Pediatr. 2016;53:883-5.
3. Scheffer IE, Berkovic S, Capovilla G, Connolly MB,
French J, Guilhoto L, et al. ILAE Classification of the
epilepsies: Position paper of the ILAE commission for classification and
terminology. Epilepsia. 2017;58:512-21.
4. Commission on classification and terminology of
the International League Against Epilepsy. Proposal for revised clinical
and electroencephalographic classification of epileptic seizures.
Epilepsia. 1981;22:489-501.
5. Commission on classification and terminology of
the International League Against Epilepsy. Proposal for revised
classification of epilepsies and epileptic synd-romes. Epilepsia. 1989;30:389-99.
6. Engel J Jr. A proposed diagnostic scheme for
people with epileptic seizures and with epilepsy: Report of the ILAE
Task Force on classification and terminology. Epilepsia.
2001;42:796-803.
7. Berg AT, Berkovic SF, Brodie MJ, Buchhalter
J, Cross JH, van Emde Boas W, et al. Revised terminology and
concepts for organization of seizures and epilepsies: Report of the ILAE
Commission on Classification and Terminology, 2005–2009. Epilepsia.
2010;51:676-85.
8. Fisher RS, Cross JH, French JA, Higurashi
N, Hirsch E, Jansen FE, et al. Operational classification of
seizure types by the international league against epilepsy: Position
paper of the ILAE commission for classification and terminology.
Epilepsia. 2017;58:522-30.
9. Fisher RS, Cross JH, Souza CD, Higurashi
N, Hirsch E, Jansen FE, et al. Instruction manual for the ILAE
2017 operational classification of seizure types. Epilepsia.
2017;58:531-42.
10. Brodie MJ, Zuberi SM, Scheffer IE, Fisher RS. The
2017 ILAE classification of seizure types and the epilepsies: What do
people with epilepsy and their caregivers need to know? Epileptic Disord.
2018;20:77-87.
|
|
|
 |
|
