|
|
|
Indian Pediatr 2013;50: 148-150
|
 |
Diagnostic Accuracy of Ultrasonic Examination
in Suspected Craniosynostosis Among Infants
|
|
Houman Alizadeh,
*Neda Najmi,
Mehrzad Mehdizade And #Nooshin
Najmi
From the Children Medical Center, Tehran University of
Medical Sciences; *Amir Alam Hospital, Tehran University of Medical
Sciences and #Imam Khomeini Hospital, Tehran University of Medical
Sciences, Tehran, Iran.
Correspondence to: Dr Neda Najmi, 2nd floor, no.8.
Izadi St. Gisha ave. Tehran. Iran.
Email: [email protected]
Received: December 19, 2011;
Initial review: January 11, 2012;
Accepted: May 04, 2012.
|
The current study was performed to assess the diagnostic accuracy of
ultrasound compared to CT scan as a gold standard in the diagnosis of
craniosynostosis. 44 infants (17 girls) under 1 year old, clinically
suspected to have craniosynostosis, were first sonographically examined
by a pediatric radiologist and were later referred to another blinded
pediatric radiologist to examine CT scan with 3D reconstructed images of
skull. Sensitivity, specificity, positive and negative predictive values
of ultrasound versus CT scan were 96.9%, 100%, 100%, and 92.3%,
respectively. The high specificity of ultrasound helps to correctly rule
out craniosynostosis in clinically suspected cases and thus, can prevent
unnecessary exposure of healthy infants to CT scan ionizing radiation.
Key words: Craniosynostosis, Diagnosis, Infants,
Ultrasonography.
|
|
C
raniosynostosis is
defined as premature fusion
of cranial sutures. It occurs in 4-6 of 10,000
live births [1]. Primary craniosynostosis is
mostly idiopathic and is due to premature fusion of cranial
sutures, while the secondary type is the result of brain
defects, including brain microcephaly or atrophy which leads to
premature fusion of the sutures [1]. In simple craniosynostosis
only one suture is involved and in compound type, more than one
suture are involved [2-4].
Craniosynostosis is traditionally diagnosed
by imaging modalities and in-time diagnosis of primary cases is
pivotal in the success of surgical treatment. Standard
radiographs are the first step in the evaluation of suspected
cases [5,6]. Presently, CT scan is considered as an alternative
to standard radiography [1]. CT scan can differentiate primary
from secondary cases of craniosynostosis by providing adequate
information about brain parenchyma. However, a major
disadvantage is the high radioactive dose [7,8], in addition to
the cost and availability issues.
Ultrasound is a non-invasive, available,
low-cost and safe modality, and is a plausible alternative to CT
scan in the diagnosis of craniosynostosis [9]. The diagnostic
accuracy of ultrasound is not established. It may even be used
for prenatal diagnosis of craniosynostosis [11]. In cases which
fontanels are open, ultrasound can reveal reliable information
about the brain structures also. The current study has been
performed to investigate the diagnostic accuracy of ultrasound
in detecting premature fusion of sutures among infants under one
year of age.
Methods
Symptomatic infants from urban areas of
Tehran were referred to Tehran Children’s Medical Center, where
they were examined by a pediatric neurologist or a pediatric
neurosurgeon. The inclusion criteria was any suspected cases who
had small head circumference or had a head skull deformity.
Informed consent was obtained from parents before inclusion of
infants in the study. From June 2007 to September 2008, 44
infants under 1 year of age, clinically suspected with
craniosynostosis, were included in the study and were examined
first by ultrasound and then by CT scan. In case the infant was
restless, chloral hydrate was administered for sedation. We did
not use oral sedation for ultrasound exams but it was
administered to 10 children for CT scan. Radiologists who
interpreted the CT scan were blinded to the diagnosis made on
ultrasound. CT scan was performed hellically with a 16 slice GE
apparatus with a thickness of 5 mm at an interval of 4 mm, and
was reconstructed with a thickness of 1.25 mm and the interval
of 1 mm before 3D-skull reconstruction. The routine condition is
KV 120 and mA 45 to 80.
All sonographic examinations were performed
using an Ultrasonix machine with a 14 MHz linear probe, in a
near field focus and with a depth of 2 cm. The probe was placed
vertically on each suture and the whole length of sutures were
evaluated. The cranial suture was considered normal in case a
hypoechoic or beveled gap between 2 hyperechoic bones was
noticed. The absence of hypoechoic gap, beveled appearance, or
the presence of ridging or bridging along the bone was
considered abnormal. Also narrow sutures, the width of which was
less than 0.5 mm, were considered as abnormal (0.5 mm is the
narrowest distance measurable by examiner). The diagnostic
criteria used have been detailed previously [12]. Data were
analyzed in SPSS version 16.0 (Chicago, IL) and the sensitivity,
specificity, positive and negative predictive values of
ultrasound were calculated.
Results
Forty four infants (17 girls) were included.
With mean age of 5 months and 23 days (SD 3 months and 13 days),
(Range, 18 days - 12 months). The mean head circumference was
41.1(SD 3.33) cm, (range, 34-47.5 cm). Only 5 infants (11.4%),
all of whom were boys, had familial history of craniosynostosis.
Delivery was normal in 16 infants (36.4%) and cesarean section
in 28 infants (63.6%). There was no difference in mean age and
mean head circumference between sexes, neither any difference in
mean head circumference between infants born normally and those
by cesarean section.
Sonographic findings: Thirteen infants
(29.5%) were recognized as healthy and 31 infants (70.5%) were
diagnosed as cases of craniosynostosis. There was no difference
in female-to-male ratio, the mean age, the mean head
circumference, and percentage of cesarean section among healthy
and unhealthy infants. Craniosynostosis was primary in 29
infants (93.5%) and secondary in 2 infants (6.5%).
Craniosynostosis was simple in 27 infants (87.1%) and compound
in 4 infants (12.9%). The most prevalent sutures involved,
ordered from high to low included: metopic, sagital, unilateral
and bilateral coronal, and bilateral lambdoid. Cranial
deformities ordered from high to low prevalence included:
trigonocephaly, scaphocephaly, brachycephaly, anterior
plagiocephaly, and posterior plagiocephaly. The brain was
abnormal in 2 infants (6.5%).
In the current study, the diagnosis of 43
infants in ultrasound was completely compatible with CT scan.
Only one patient diagnosed in CT scan was missed in ultrasound.
The patient was a boy with 7 and half months of age, with
positive family history, and born by cesarean section. The boy
had primary compound craniosynostosis detected in CT scan,
involving both sagital and metopic sutures who presented with
scaphocephaly. In CT scan, bridging was noticed along 4 cm of
the suture. The brain was reported to be normal.
The sensitivity, specificity, positive and
negative predictive values of ultrasound versus CT scan were
96.9%, 100%, 100%, and 92.3%, respectively. There was no
significant difference in diagnostic accuracy of ultrasound
between girls and boys, and between infants under 6 months and
infants older than 6 months (Table I).
TABLE I Diagnostic Characteristics Of Ultrasound Compared To CT Scan
| |
Gender |
Age |
|
Female (n=17) |
Male (n=27) |
< 6 mo (n=26) |
>6 mo (n=18)
|
Total |
|
Sensitivity (95% CI) |
100%
|
95.2% |
100% |
90.9% |
96.9% |
|
(97.0%-100%) |
(90.5%-99.9%) |
(97.8%-100%) |
(81.8%-100%) |
(93.8%-100%) |
|
Specificity (95% CI) |
100% |
100% |
100% |
100% |
100% |
|
(95.9%-100%) |
(95.9%-100%) |
(96.3%-100%) |
(95.6%-100%) |
(97.1%-100%) |
|
Positive Predictive Value (95% CI) |
100% |
100% |
100% |
100% |
100% |
|
(97.0-100%) |
(97.8%-100%) |
(97.8%-100%) |
(96.9%-100%) |
(98.2%-100%) |
|
Negative Predictive Value (95% CI) |
100% |
85.7% |
100% |
83.3% |
92.3% |
|
(95.9%-100%) |
(71.4%-100%) |
(96.3%-100%) |
(66.6%-100%) |
(84.7%-99.9%) |
|
CI: Confidence Interval.
|
Discussion
The higher prevalence of simple
craniosynostosis than compound type, and primary than secondary
type is concordant with previous studies [1,2]. It may be a
referral bias, as primary cases of craniosynostosis are more
frequently referred to Children’s Medical Center than secondary
cases, because primary cases can be surgically treated. The
relative frequency of sutures involved and of various types of
cranial deformities was not concordant with previous studies
[13]. One possible justification is that scaphocephaly is not
considered as a skull deformity among general public, and that’s
why most referred infants present with trigonocephaly.
 |
|
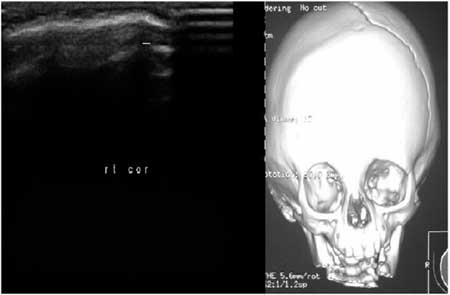
Fig.1 (a) Sonographic image
and (b) CT scan image of a one-month old female infant
with right coronal synostosis and plagiocephaly.
|
We emphasize the high negative predictive
value of ultrasound compared to CT scan. Ultrasound can be
suggested as the preferred screening method for craniosynostosis
as many patients will be thus spared from unnecessary exposure
to ionizing radiation, as also suggested earlier [14]. The
accuracy reported in previous studies is even higher that the
current study [10,12,14]. Moreover, ultrasound is capable of
diagnosing prenatal craniosynostosis [11]. However, it should be
noted that ultrasound is operator-dependent and radiologists
should be specifically trained to detect craniosynostosis by
using ultrasound [15].
The overall accuracy of ultrasound justifies
its applicability in the diagnosis of craniosynostosis. Based on
the results of this study, we can conclude that ultrasound can
be a low-cost and accurate alternative to CT scan, especially
the preferred screening method in infants clinically suspected
to primary simple or complex craniosynostosis.
Contributors: HA and NN: conceived
designed the study, collected the data, drafted the paper and
revised the manuscript for important intellectual content; NN:
will act as guarantor of the study; MM: revised the manuscript
for important intellectual content and helped in manuscript
writing and NN analyzed the data and helped in manuscript
writing. The final manuscript was approved by all authors.
Funding: Research Center of Children
Medical Center, Tehran University of Medical Science, Tehran,
Iran.
Competing interests: None stated.
Refrences
1. Kotrikova B, Krempien R, Freier K, Muhling
J. Diagnostic imaging in the management of craniosynostoses. Eur
Radiol. 2007;17:1968-78.
2. Khan M. Craniosynostosis. eMedicine
Specialties. 2007;14:233-5.
3. Aldridge K, Marsh JL, Govier D,
Richtsmeier JT. Central nervous system phenotypes in
craniosynostosis. J Anat. 2002;201:31-9.
4. Junger TH, Reicherts M, Steinberger D,
Collmann H, Kotrikova B, Zoller J, et al. Standardized
evaluation and documentation of findings in patients with
craniosynostosis. J Maxillofac Surg. 2001;29:25-32.
5. Aviv RI, Rodger E, Hall CM.
Craniosynostosis. Clin Radiol. 2002;57:93-102.
6. Tang TT, McLeary MS. Imaging of the
cranium: pictorial essay. Acad Radiol. 1999;6:132-40.
7. Tokumaru AM, Barkovich AJ, Ciricillo SF,
Edwards MS. Skull base and calvarial deformities:
association with intracranial changes in craniofacial syndromes.
AJNR Am J Neuroradiol. 1996;17:619-30.
8. Domeshek LF, Mukundan S, Jr., Yoshizumi T,
Marcus JR. Increasing concern regarding computed tomography
irradiation in craniofacial surgery. Plast Reconstr Surg.
2009;123:1313-20.
9. Sze RW, Parisi MT, Sidhu M, Paladin AM,
Ngo AV, Seidel KD, et al. Ultrasound screening of the
lambdoid suture in the child with posterior plagiocephaly.
Pediatr Radiol. 2003;33:630-6.
10. Soboleski D, McCloskey D, Mussari B,
Sauerbrei E, Clarke M, Fletcher A. Sonography of normal
cranial sutures. AJR Am J Roentgenol. 1997;168:819-21.
11. Stelnicki EJ, Mooney MP, Losken HW,
Zoldos J, Burrows AM, Kapucu R, et al. Ultrasonic
prenatal diagnosis of coronal suture synostosis. J Craniofac
Surg. 1997;8:252-8; discussion 259-61.
12. Regelsberger J, Delling G, Helmke K,
Tsokos M, Kammler G, Kranzlein H, et al. Ultrasound in
the diagnosis of craniosynostosis. J Craniofac Surg.
2006;17:623-5; discussion 626-8.
13. Ploplys EA, Hopper RA, Muzaffar AR, Starr
JR, Avellino AM, Cunningham ML, et al. Comparison of
computed tomographic imaging measurements with clinical findings
in children with unilateral lambdoid synostosis. Plast
Reconstr Surg. 2009;123:300-9.
14. Simanovsky N, Hiller N, Koplewitz B,
Rozovsky K. Effectiveness of ultrasonographic evaluation of the
cranial sutures in children with suspected craniosynostosis. Eur
Radiol. 2009;19:687-92.
15. Ngo AV, Sze RW, Parisi MT, Sidhu M,
Paladin AM, Weinberger E, et al. Cranial suture simulator
for ultrasound diagnosis of craniosynostosis. Pediatr Radiol.
2004;34:535-40.
|
|
|
 |
|
