|
|
|
Indian Pediatr 2011;48: 62-63 |
 |
Giant Condyloma Acuminata in Pediatric HIV |
|
Rita Chatterjee, Subhasish Bhattacharyya, Rupa Biswas and Shubhadeep Das
From the Department of Pediatric Medicine and Regional
Pediatric ART Center, Medical College, Kolkata, India.
Correspondence to: Dr Rita Chatterjee, 3C, Bakul Bagan
Row Bhowanipore, Kolkata 700 025,
West Bengal, India.
Email: [email protected]
Received: March 2, 2009;
Initial review: April 15, 2009;
Accepted: August 18, 2009.
|
We report a 2 year 6 months old girl suffering from HIV infection and
presenting with two giant condyloma acuminata of perianal and perivulvar
region along with oral candidiasis.
Key words: Giant condyloma acuminata, Pediatric HIV.
|
|
HPV
(human papillomavirus) infection has been shown to occur in about 8-10% of
pediatric HIV patients. A variety of HPV show different clinical
manifestations. Of the many subtypes, the mucosal type, condyloma
acuminata has been observed more frequently in HIV infected children and
tends to occur in the anogenital region [1,2]. But a large condyloma
acuminata as the dominant manifestation of pediatric HIV is rarely
reported.
Case Report
A 2 year-6 months-old female child presented with
reddish brown huge perianal and perivulvar growth. The growth had started
as warty lesions around the anus and vulval opening 4 months back and had
grown in size and coalesced to assume huge dimensions. She also had
difficulty in swallowing for 7 days, and fever for 4 days. There was
history of her father’s premature death 1 year back, the cause of which
was unknown. There was no history of sexual abuse with the child. On
examination, she was cachectic, pale, and having Grade IV malnutrition (IAP).
There were multiple enlarged and tender cervical lymph nodes along with
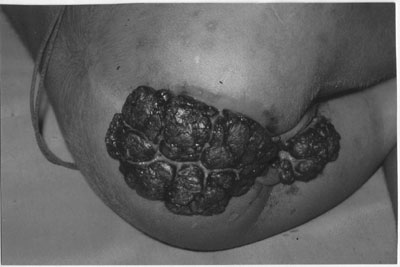
tachypnea. The perianal growth measured 8x10 cm with a thickness of 2.5 cm
at the centre, while the perivulvar growth measured 6×5 cm (Fig.
1). The lesions were cauliflower like, fleshy, sessile, slightly
friable at certain areas with few bleeding points. There were creamy white
plaques on the dorsal surface of the tongue, palate and buccal mucosa.
Other systemic examination findings were essentially normal. The child’s
mother did not have any skin or genital warts. Her hemoglobin was 5g/dL,
platelet count was 40,000/cmm, and TLC was normal. Chest radiograph
revealed right sided pneumonitis. Mantoux test was negative. Patient was
tested HIV ELISA positive but VDRL negative. The CD4 count was 150/cu mm.
Her mother was also positive for HIV. Histopathological examination
(biopsy) showed koilocytosis, hyperkeratosis and acanthosis, typical of
condyloma acuminata without any features of malignancy. Patches were
scraped off from the mouth, microscopic examination of KOH smear showed
pseudohyphae and blastospores. A final diagnosis of pediatric HIV
presenting with giant perianal and perivulvar condyloma acuminata along
with oral candidiasis, was made and the girl was initiated on broad
spectrum antibiotics, fluconazole, co-trimoxazole. Anti retroviral therapy
was also started simultaneously. However, the girl died on the 7th day of
her admission.
 |
|
Fig. 1 Huge cauliflower like perianal and
perivulvar giant condyloma acuminata in a 2 years 6 months old girl
child. |
Discussion
Our patient was suffering from HIV infection and
reported at our OPD mainly for giant condyloma acuminata. She had probably
acquired the infection perinatally from the mother.
Modes of transmission of HPV in children remain
controversial. These include perinatal transmission, autinoculation and
heteroinoculation, sexual abuse, indirect transmission via contact through
fomites, etc. Newborn babies can be exposed to cervical HPV infection of
the mother during delivery. In-utero transmission to the fetus may
occur hematogenously, by semen fertilization, or as an ascending infection
in the mother [3,4]. Because "skin" HPV types (usually HPV type 2)
commonly are reported in cases of anogenital warts in children older than
4 years of age, typing a specific HPV associated with a particular
anogenital wart is not definitive of sexual abuse. Conversely, the
"genital" HPV types (types 6 and 11) are common in children younger than 3
years of age, even in children for whom sexual abuse is not suspected.
Exposure in these younger children probably occurs during passage through
their mother’s HPV-infected birth canal.
The presence of anogenital warts in a child is not a
reliable indicator of sexual abuse, and typing the specific HPV associated
with a particular anogenital wart also is not indicative of sexual abuse
[5]. The incubation period varies from 2-8 months. Only a small portion of
those infected with HPV express the disease [6]. Diagnosis of HPV
infections is usually clinical. Biopsies are rarely required to rule out
malignancies associated with such infections. These lesions are treated
with cryotherapy using nitrogen, Nd:Yag laser, topical agents such as
trichloroacetic or salicylic acid, podophyllin, podophyllotoxin, imiquimod,
or ablative surgery [7].
Contributors: RC: Guarantor, overall
coordinator, manuscript writing and revising it critically; SB:
conception, manuscript writing and critical revision; RB: writing the
manuscript; SD: drafting of the manuscript.
Funding: None.
Competing interests: None stated.
References
1. Straka BF, Whitaker DL, Morrison SH. Cutaneous
manifestations of acquired human immunodeficiency syndrome in children. J
Am Acad Dermatol. 1988;18: 1089-1102.
2. Forman A, Prendiville J. Association of human
immunodeficiency virus seropositivity and extensive perineal condylomata
acuminata in a child. Arch Dermatol. 1988;124:1010-1.
3. Rivera A, Tyring SK. Therapy of cutaneous human
papilloma virus infections. Dermatol Ther. 2004;17:441-8.
4. Syrjanen S, Puranen M. Human papillomavirus
infections in children: the potential role of maternal transmission. Crit
Rev Oral Biol Med. 2000;11:259-74.
5. Oriel JD. Sexually transmitted diseases in children:
human papillomavirus infection. Genitourin Med. 1992;68:80-3.
6. Bouscarat F, Mahe E, Descamps V. External anogenital
condylomas. Ann Dermatol Venereol. 2002;129:1013-2.
7. Drake LA, Dineheart SM, Farmer ER. Guidelines of
care for warts: Human papilloma virus. J Am Acad Dermatol. 1995;32:98-103.
|
|
|
 |
|
