|
|
|
Indian Pediatr 2011;48: 25-30 |
 |
Clinical Screening for Congenital Heart
Disease at Birth: A Prospective Study in a Community Hospital in
Kerala |
|
Balu Vaidyanathan, Gayathri Sathish, Sinimol Thoppil Mohanan, Karimassery
Ramaiyar Sundaram*,
Karukappilly Krishnan Raghava Warrier† and Raman Krishna Kumar
From the Departments of Pediatric Cardiology and
*Biostatistics, Amrita Institute of Medical Sciences and Research Center,
AIMS Ponekkara PO, and †Department of Pediatrics, Lakshmi Hospital, Kochi,
Kerala, India.
Correspondence to: Dr Balu Vaidyanathan, Clinical
Professor, Pediatric Cardiology, Amrita Institute of Medical Sciences,
AIMS Ponekkara PO, Kochi, Kerala, 682 041, India.
Email:
[email protected]
Received: December 14, 2009 ;
Accepted: January 29, 2010.
Published online: 2010 August 1.
PII:
S097475590900878-1
|
|
Abstract
Objective: To develop a clinical strategy for
detection of Congenital heart disease (CHD) in the newborn through a
combination of clinical signs and pulse oximetry.
Design: Prospective longitudinal study.
Setting: Community level hospital in the city of
Kochi, Kerala.
Participants and interventions: All consecutive
newborns between June 2006 and February 2009 were prospectively screened
for CHD, 48 hours after birth. The on-site pediatrician performed
clinical screening. A study nurse recorded pulse oximetry in a lower
extremity; value of <94% was defined as abnormal. Echocardiography was
performed on site by a trained research officer. A 6-week clinical
follow-up evaluation was done for all.
Main outcome measure: Detection of CHD by
echocardiography.
Results: Of 5487 babies screened, 425 (7.75%) had
CHD. 17 (0.31%) had major CHD, two of whom (one ALCAPA and one large VSD)
were missed during the initial evaluation. The rest were minor CHD (408
patients, 7.44%), most of which normalized by 6 weeks. On multivariate
analysis, murmur, central cyanosis, abnormal precordial pulsations and
abnormal pulse oximetry emerged as significant predictors of CHD. The
sensitivity of clinical evaluation and pulse oximetry combined was 19%
for all CHDs and 20% for major CHD; specificity was 88%.
Conclusions: In the community setting of a
developing country, clinical evaluation and pulse oximetry after birth
had a very low sensitivity for detection of CHD. Though an abnormal
screening warrants prompt echocardiography, a 6-week clinical evaluation
is recommended to ensure that major CHD is not missed.
Key words: Congenital heart disease, India, Newborn, Pulse
oximetry, Screening.
|
|
C
ongenital heart diseases (CHD)
account for about 10% of infant deaths and about half of deaths due to
congenital malformations in developed countries [1]. The prevalence of CHD
diagnosed in the first 12 months is estimated at 6-8 per 1000 live births
[2]. About 25% of CHDs are life-threatening and may manifest before the
first routine clinical examination [3,4]. Failure to identify these
critical lesions immediately after birth leads to delay in referral and
increased mortality and morbidity [5]. Several studies have documented the
lack of sensitivity of routine neonatal examination in detecting CHD
[6-10]. Recent studies have reported a high sensitivity and specificity
for pulse oximetry for early detection of CHD in newborn babies [11-16].
Combining pulse oximetry with clinical examination can enhance the
clinician’s ability to detect life-threatening CHD in a timely manner
[17,18].
With advances in perinatal care, congenital
malformations are emerging as one of the leading causes of neonatal and
infant mortality, even in developing countries [19]. Challenges for CHD
management in developing countries include early diagnosis, transport of a
sick neonate with CHD to a tertiary cardiac center, and limited
availability of state-of-the-art pediatric cardiac centers [20]. The
present study, conducted in a community hospital, attempted to identify a
strategy based on clinical signs and pulse oximetry that best predicts CHD
in newborns immediately after birth.
Methods
This was a prospective hospital-based study (June
2006-February 2009) conducted in a secondary level hospital (Lakshmi
hospital) in Kochi, Kerala. The study personnel were given one-month
training at the coordinating centre (Amrita Institute of Medical
Sciences). All consecutive babies (including pre-mature infants) were
screened for CHD according to a pre-designed protocol. Out-born babies
were excluded. Clinical evaluation was performed by the on-site
pediatrician within the first 48 hours of life. Pulse oximetry was
recorded in a lower extremity by a study nurse using portable equipment (Oximax
N-65; Nellcor Puritan Bennett, Pleasanton, CA) at 48 hours after
birth. Bedside echocardiography was done by the research officer, using a
portable machine (Cyprus-Acuson, Siemens Medical Solutions, USA). All
babies with abnormal bedside echo-cardiography were evaluated by a
pediatric cardiologist (major CHD – immediately; minor CHD – at 6 weeks).
For the normal babies, a follow-up evaluation (clinical evaluation,
questionnaire or telephonic interview of parents) was performed at 6
weeks. If this was abnormal, echocardiography was repeated.
Definitions of CHD: Patients were categorized into
those with and without CHD based on echocardiography [2]. Any CHD that was
likely to require early intervention was categorized as major CHD. Minor
CHD was defined as any atrial septal defect (ASD) >5mm, patent ductus
arteriosus (PDA) >2mm, restrictive ventricular septal defect (VSD) with
gradient >30mm Hg, valvular aortic/pulmonary stenosis with gradients <25
mm Hg, and pulmonary artery branch stenosis with gradients <20 mm Hg. All
others (including patent foramen ovale or ASD <5 mm, PDA <2 mm) were
categorized as normal variants. Abnormal pulse oximetry was defined as
oxygen saturation <94% [11].
Statistical analysis: For analysis, all
patients with CHD, including the ones detected during follow-up were
considered. Univariate analysis was performed using Chi-square test. All
variables which were significant with P <0.2 (80% confidence) were
entered into a stepwise logistic regression model for multivariate
analysis. Results were expressed as Odd’ ratios for association with CHD
(with 95% confidence limits) as well as P values. P value of
<0.05 was considered significant. Sensitivity, specificity, positive and
negative predictive values were computed for clinical signs, pulse
oximetry and echocardiography.
An informed consent was obtained from one of the
parents before initial screening. The study protocol was approved by the
ethics committees of the Institute and the Indian Council of Medical
Research.
Results
A total of 5487 consecutive newborn babies were
included in the study. Of these, 5086 (92.7 %) were well babies and 401
(7.3%) required admission in the neonatal intensive care unit. 2688 (49%)
were males. The mean birthweight was 2.93 ± 0.53 Kg. Table I
summarizes the baseline demographic characteristics of the study
population.
TABLE I
Baseline Characteristics of the Study Population
| Variable |
Number (%) |
| Gestational age: Term |
4940 (90.3) |
| Pre-term |
528 (9.7) |
| Family history of CHD |
43 (0.8) |
| Consanguinity |
107 (2) |
| Maternal diabetes mellitus |
542 (10) |
| Pregnancy induced hypertension |
571 (10.6) |
| Infections during pregnancy |
264 (4.9) |
| Exposure to teratogenic drugs |
18 (0.3) |
| Parental smoking |
672 (12.5) |
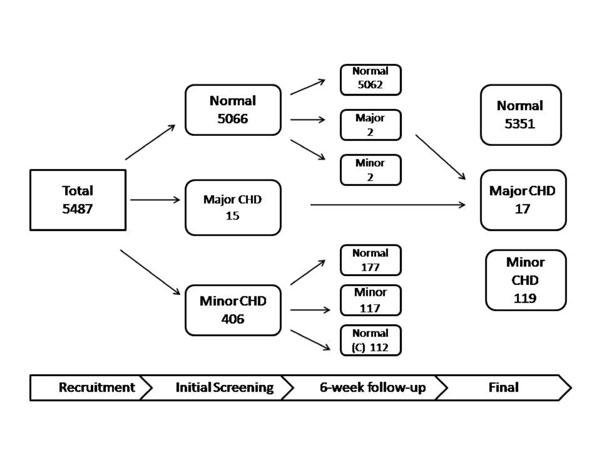
A CHD was detected in 425 neonates (7.75%). Seventeen
patients (0.31%) were classified as major (large perimembranous VSD 5,
sinus venosus ASD 2, large PDA 2, dTGA 2, Tetralogy of Fallot 2, Primum
ASD 1, double aortic arch 1; the rest (408 patients, 7.44%) were minor CHD.
Four patients were detected during the 6-week follow-up evaluation. Two of
these had major CHD, presenting with heart failure between 4-6 weeks of
age (1, anomalous left coronary from the pulmonary artery, requiring
surgery and 1, large VSD). Two other patients presented with asymptomatic
murmur at 6 weeks (both had moderate sized ASDs). Majority (71.3%) of the
minor CHDs normalized by 6-weeks follow-up. Fig. 1
summarizes the findings of the initial screening and 6-week follow-up.
 |
|
Fig. 1 Details of CHD diagnosed on initial
screening and 6-week follow-up. |
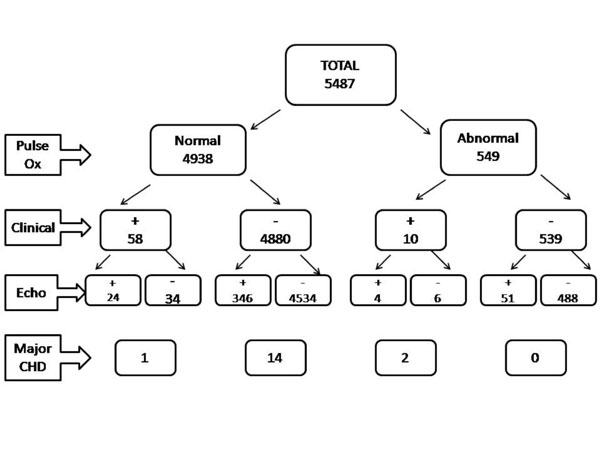
A total of 157 patients (2.9%) had positive clinical
evaluation, the most common being murmur (84 patients, 1.6%). Clinical
evaluation was positive in only 3 patients (17.6%) with major and 32
patients (7.8%) with minor CHD. Abnormal pulse oximetry was found in 549
(10%) patients, of which 55 (10%) had CHD on echocardiography (2 major, 53
minor). Abnormal pulse oximetry was detected in only 2 patients (11.8%)
with major CHD; 4 whereas four patients had cyanotic CHDs. 53 patients
with minor CHD (none with cyanotic CHD) had abnormal pulse oximetry.
Figure II summarizes the results of pulse oximetry and
its association with clinical signs and echocardiography.
 |
|
Fig. 2 Association of pulse oximetry with
clinical evaluation and echocardiography. |
The overall sensitivity for the clinical signs and
abnormal pulse oximetry combined was 19% for all CHDs and 20% for major
CHD. (Table II). Fourteen patients (82.3%) with major CHD
had normal clinical evaluation and pulse oximetry. Bedside
echocardiography had a sensitivity, specificity and negative predictive
value of 88.2%, 92.6% and 99.9%, respectively for major CHD.
TABLE II
Sensitivity, Specificity, and Positive and Negative Predictive Value of Clinical Signs
|
Variable |
All CHDs |
Major CHDs |
| |
Sensitivity |
Specificity |
PPV |
NPV |
Sensitivity |
Specificity |
PPV |
NPV |
|
Clinical |
9.26 |
97.4 |
23.3 |
92.8 |
13.3 |
96.9 |
1.1 |
99.7 |
|
Pulse oximetry |
11.4 |
90.9 |
9.4 |
92.8 |
13.3 |
90.7 |
0.3 |
99.7 |
|
Combined |
19 |
88 |
12 |
92 |
20 |
87.9 |
0.4 |
99.7 |
CHD: congenital heart disease, NPV: negative predictive value, PPV: positive predictive value; All values in percentage.
|
On univariate analysis, maternal diabetes mellitus (O.R
1.39, 95% C.I 1.03-1.89; P=0.029), family history of CHD (O.R 2.37,
95% C.I 1.04-5.35; P = 0.05), history of ante-natal exposure to
teratogenic drugs (O.R 3.47, 95% C.I 1.14-10.64; P 0.05), murmur (O.R
24.39, 95% CI 3.62-9.35, P <0.001), respiratory distress( OR 2.76;
95% CI 1.27-5.99, P <0.017), central cyanosis ( OR 8.18, 95% CI
1.37-50, P 0.05), abnormal precordial pulsations( O.R 24.39, 95%
C.I 3.62-9.35, P 0.005) and abnormal pulse oximetry ( OR 1.39, 95%
CI 1.01-1.91, P <0.042) were found to be significantly associated
with all CHD. The results of multivariate analysis are summarized in
Table III.
TABLE III
Multivariate Analysis of Predictors of CHD
|
Variable |
Odds ratio (95% CI) |
P value |
|
Murmur |
5.61 (3.31-9.52) |
<0.001 |
|
Central cyanosis |
15.52 (1.22-197.6) |
0.035 |
|
Abnormal precordial pulsations |
20.22 (1.55-263.21) |
0.022 |
|
Abnormal pulse oximetry |
1.41(1.01-1.97) |
0.047 |
|
Male sex |
1.3 (1.04-1.62) |
0.021 |
|
Family history of CHD |
2.74 (1.19-6.29) |
0.018 |
|
CHD: Congenital
heart disease. |
Discussion
The results of this study bring out the inherent
limitations of clinical screening for CHD in newborns immediately after
birth, especially in the context of limited resource environments. The
overall prevalence of CHD reported in this study is higher than that
reported previously from various population-based studies [2]. This is
accountable by the detection of minor, self- resolving lesions due to use
of echocardiography for screening all babies. Though murmur, cyanosis and
abnormal pulse oximetry were identified as predictors of CHD, the
sensitivity of these signs to detect CHD were very low (combined clinical
evaluation and pulse oximetry had a sensitivity of <20%).
Previous studies have reported low sensitivity of
clinical examination for detection of CHD in the newborn [4-10]. This
study reports a poor sensitivity for pulse oximetry, as well, for
detection of CHD [11-17]. Pulse oximetry was also found to have a low
predictive value. This may be due to the fact that only four patients in
this study had critical CHD with cyanosis. In addition, technical and
human factors may also have contributed to the low sensitivity of pulse
oximetry, as previously reported [21]. Hence, repeated testing and
adequate training of manpower is required before pulse oximetry can be
recommended for clinical screening of CHD on a mass level [22]. These
issues may limit the widespread use of pulse oximetry as a screening tool
for CHD in developing countries.
Though echocardiography is the gold standard for
diagnosis of CHD and can be performed by neonatologists with acceptable
accuracy, it is not feasible as a routine screening tool, especially in
developing countries [23-25]. In this study, even after echocardiography,
two patients with major CHD, including a potentially life threatening
condition ALCAPA, were missed after the initial screening. This
demonstrates the limitations of echocardiography for detection of CHD in
the neonates, especially when performed by personnel with limited
training, and its potential pitfalls in picking up critical lesions like
congenital coronary abnormalities before symptoms have set in.
This study suggests that the presence of abnormal
clinical signs like murmur should warrant a prompt cardiac evaluation.
With training and repeated testing, pulse oximetry may potentially emerge
as a useful adjunct to clinical evaluation, especially for cyanotic CHD.
Even if the initial screening is normal, it is mandatory to have a
follow-up clinical evaluation at 6 weeks. A comprehensive approach
consisting of improved awareness, refining of clinical skills and training
of personnel in newer diagnostic techniques (pulse oximetry and
echocardiography) is required to ensure that major CHDs do not go
undetected in the newborn before discharge from hospital. Large studies
are needed for testing the conclusions derived from this study.
This study did not address the impact of fetal
echocardiography on the prevalence of major CHD in the population studied.
It is possible that the most complex forms of CHDs may have been
terminated after a prenatal diagnosis. A follow-up echocardiogram at 6
weeks was not routinely performed for most patients with minor CHD as well
as those with normal screening.
In the community setting of a developing country,
clinical evaluation and pulse oximetry after birth had a very low
sensitivity for detection of CHD. Though an abnormal screening warrants
prompt echocardiography, a 6-week clinical evaluation is recommended to
ensure that major CHD is not missed.
Contributors: BV designed the study, analyzed the
data and wrote the manuscript and shall act as the guarantor for the
paper; GS collected the data, helped in data analysis and manuscript
preparation; STM collected the data and helped in analysis; KRS performed
the statistical analysis; KKRV critically reviewed the manuscript, and RKK
designed the study and critically reviewed the manuscript.
Funding: This study was supported by a research
grant from the Indian Council of Medical Research, New Delhi, India and a
grant from Children’s Heart Link, Minneapolis, USA.
Competing interest: None stated.
|
What Is Already Known?
• Clinical evaluation has a very low sensitivity
for detection of CHD in asymptomatic newborns.
What This Study Adds?
• In the setting of low resource environments,
the utility of pulse oximetry as a screening tool for CHD is
limited.
• Training of personnel in the technique of pulse
oximetry is essential before it can be recommended for mass
screening for CHD in developing countries.
|
References
1. Abu-Harb M, Hey E, Wren C. Death in infancy from
unrecognized congenital heart disease. Arch Dis Child. 1994;71: 3-7.
2. Hoffman JIE, Kaplan S. The incidence of congenital
heart disease. JACC. 2002;39:1890-900.
3. Wren C, Reinhardt Z, Khawaja K. Twenty-year trends
in diagnosis of life-threatening neonatal cardiovascular malformations.
Arch Dis Child Fetal Neonatal Ed. 2008; 93:F33-F35.
4. Richmond S, Wren C. Early diagnosis of congenital
heart disease. Semin Neonatol. 2001;6:27-35.
5. Keuhl KS, Loffredo CA, Ferencz C. Failure to
diagnose congenital heart disease in infancy. Pediatrics. 1999; 103:
743-7.
6. Meberg A, Otterstad JE, Froland G, Hals J, Sorland
SJ. Early clinical screening of neonates for congenital heart disease: the
cases we miss. Cardiology Young.1999; 9: 169-74.
7. Lee TW, Skelton RE, Skene C. Routine neonatal
examination: Effectiveness of trainee pediatrician compared with advanced
neonatal nurse practitioner. Arch Dis Child Fetal Neonatal Ed. 2001; 85:
F100-4.
8. Wren C, Richmond S, Donaldson L. Presentation of
congenital heart disease in infancy: implications for routine examination.
Arch Dis Child Fetal Neonatal Ed. 1999;80: F49-F53.
9. Ainsworth SB, Wyllie JP, Wren C. Prevalence and
clinical significance of cardiac murmurs in neonates. Arch Dis Child Fetal
Neonatal Ed. 1999; 80: F43-F45.
10. Arlettaz R, Archer N, Wilkinson AR. Natural history
of innocent heart murmurs in newborn babies: controlled echocardiographic
study. Arch Dis Child. 1998;78:F166-F170.
11. Koppel RI, Druschel CM, Carter T, Goldberg BE,
Mehta PN, Talwar R, et al. Effectiveness of pulse oximetry
screening for congenital heart disease in asymptomatic newborns.
Pediatrics. 2003;111:451-5.
12. Reich JD, Miller S, Brogdon B, Casatelli J, Gomph
T, Huhta JC, et al. The use of pulse oximetry to detect congenital
heart disease. J Pediatr. 2003;142:268-72.
13. Richmond S, Reay G, Abu-Harb M. Routine pulse
oximetry in the asymptomatic newborn. Arch Dis Child Fetal Neonatal Ed.
2002;87:F83-8.
14. Hoke TR, Donohue PK, Bawa PK, Mitchell RD, Pathak
A, Rowe PC, et al. Oxygen saturation as a screening test for
critical congenital heart disease: A preliminary study. Pediatr Cardiol.
2002;23:403-9.
15. Meberg A, Brugmann-Pieper S, Due R Jr, Eskedal L,
Fageru I, Farstad T, et al. First day of life pulse oximetry
screening to detect congenital heart defects. J Pediatr. 2008;152:761-5.
16. Bakr AF, Habib HS. Combining pulse oximetry and
clinical examination in screening for congenital heart disease. Pediatr
Cardiol. 2005;26:832-5.
17. Arlettaz R, Bauschatz AS, Monkoff M, Essers B,
Bauersfeld U. The contribution of pulse oximetry for early diagnosis of
congenital heart disease in newborns. Eur J Pediatr. 2006;165:94-8.
18. Singh M. Care of the Newborn. 5th Edition. New
Delhi: Sagar Publications; 2004.
19. Kumar RK, Shrivastava S. Pediatric heart care in
India. Heart. 2008;94: 984-90.
20. Bakshi KD, Vaidyanathan B, Sundaram KR, Roth SJ,
Shivaprakasha K, Rao SG, et al.. Determinants of early outcome
after neonatal heart surgery in a developing country. J Thoracic Cardio
Vascular Surgery. 2007;134: 765-71.
21. Reich JD, Connolly B, Bradley G, Litman S, Koeppel
W, Lewycky P. Reliability of a single pulse oximetry reading as a
screening test for congenital heart disease in otherwise asymptomatic
newborn infants: The importance of human factors. Pediatr Cardiol.
2008;29:371-6.
22. Mahle WT, Newburger JW, Matherne GP, Smith FC, Hoke
TR, Koppel R, et al. Role of pulse oximetry in examining newborns
for congenital heart disease. A scientific statement from the American
Heart Association and American Academy of Pediatrics. Circulation.
2009;120: 447-8.
23. Evans N. Echocardiography on neonatal intensive
care units in Australia and New Zealand. J Paediatr Child Health.
2000;36:169-71.
24. Katumba-Lunyenya JL. Neonatal/infant
echocardiography by the non-cardiologist: a personal practice, past,
present, and future. Arch Dis Child Fetal Neonatal Ed. 2002; 86: F55-7.
25. Skinner JR. Echocardiography on the neonatal unit:
a job for the neonatologist or cardiologist. Arch Dis Child 1998;78:401-2.
|
|
|
 |
|
