|
|
|
Indian Pediatr 2009;46: 23-28 |
 |
Effect of Sling Application on Efficacy of
Phototherapy in Healthy Term Neonates with Non-hemolytic
Jaundice: A Randomized Conrolled Trial |
|
Sindhu Sivanandan, Deepak Chawla, Satish Misra, Ramesh
Agarwal and Ashok K Deorari
From Division of Neonatology, WHO Collaborating Centre
for Training and Research in Newborn Care,
Department of Pediatrics, All India Institute of Medical Sciences, New
Delhi 110 029, India.
Correspondence to: Dr. Ashok Deorari, Professor,
Department of Pediatrics, Division of Neonatology,
Coordinator, WHO-CC for Training and Research in Newborn Care, All India
Institute of Medical Sciences,
Ansari Nagar, New Delhi 110 029. E-mail:
[email protected]
Manuscript received: August 28, 2007;
Initial review completed: December 20, 2007;
Revision accepted: April 26, 2008. |
|
Abstract
Objective : To
evaluate the efficacy of white reflecting material (slings) hung from the
sides of compact fluorescent lamp (CFL) phototherapy equipment in reducing
the duration of phototherapy in healthy term neonates with non-hemolytic
jaundice.
Design: Randomized controlled trial.
Setting: Postnatal ward of a tertiary level
neonatal unit.
Participants and intervention: Healthy term
neonates with non-hemolytic jaundice between 24 hours and 10 days of age
were randomly assigned to receive single surface phototherapy with (n=42)
or without slings (n=42).
Outcome measure: Duration of phototherapy in hours
(h) and the requirement of exchange transfusion.
Results: Birthweight (2790±352 vs. 2923±330 g),
gestation (38±1.3 vs. 37 ±1.0 wk) and
initial serum total bilirubin (STB) (16.6±2.4 vs. 16.1±2.2 mg/dL) were
comparable between the two groups. There was no significant difference in
the duration of phototherapy (mean±SD) between the Sling (23.3±12.9 h) and
No sling (24.9±15.4h) groups (P=0.6). The irradiance of photo-therapy
equipment (microwatt/cm2, mean±SD) was higher in Sling group compared to
No sling group (195.8± 24.2 versus 179.7±27.7, P=0.01). There was a trend
towards a higher rate of fall of serum total bilirubin (mg/dL, mean±SD) in
the Sling group (0.23±0.49) compared to No sling group (0.03±0.47)
(P=0.06).
Conclusion: Though hanging of white reflective
sling on sides of CFL phototherapy equipment resulted in marginal increase
in irradiance, it did not decrease the duration of phototherapy.
Key words: Hyperbilirubinemia, Neonate, Phototherapy, Slings. |
|
P
hototherapy is the single most
common intervention used for treatment of neonatal jaundice(1). The
therapeutic efficacy of phototherapy can be enhanced by use of special
blue light and by employing "Double-surface" phototherapy units(2-5). A
sling made of reflective material, hung on the sides of a phototherapy
unit may also increase the exposed body surface area by reflecting light
and therefore, can increase the efficacy of phototherapy(6-8). Although
use of white reflective material has been recommended to achieve faster
decline of serum bilirubin(2), use of slings for this purpose has not been
investigated adequately.The objective of our study was to evaluate
whether, the use of white reflecting material hung on sides of a
phototherapy unit increases the efficacy of phototherapy in term neonates
with non-hemolytic jaundice.
Methods
Subjects: All term ( ³37
wk) neonates born in the hospital between October 2005 and March 2007 were
eligible for enrollment if they satisfied the following criteria: age >24
hour (h) and £10
days, Apgar at 5 min greater than 6 and serum total bilirubin (STB) less
than 21 mg/dL. Exclusion criteria were hyper-bilirubinemia requiring
exchange transfusion, Rh hemolytic disease, evidence of hemolysis in
peripheral smear, positive direct Coomb’s test (DCT), glucose-6-phosphate
dehydrogenase (G6PD) deficiency, major congenital malformation,
culture-positive sepsis and need of intensive care .
Intervention and randomization: All term
neonates born during the study period were clinically monitored for the
development of jaundice. STB was measured as per judgment of treating
team. The decision to start phototherapy was based on AAP guidelines for
term and near-term babies(2). The eligible infants were randomized by
sealed, serially numbered, opaque envelopes to single compact fluorescent
light (CFL) phototherapy unit either with or without slings. The
phototherapy units (Model CFL 100, M/s Phoenix Medical System Private
Limited, India) were fitted with six light sources (Osram Dulux L 18W/71),
four blue CFLs and two white CFLs. Two such phototherapy units were
designated to be used exclusively for the study and the white-reflecting
material could be hung to any of these units by Velcro strips. This method
ensured that the same phototherapy unit could be used with or without
slings. The slings were made up of white plastic sheets with reflecting
inner surface. The slings covered three sides of the unit. The one side
was left open for uninterrupted observation of the neonate. The
phototherapy was administered in the postnatal wards on the mothers’ cots.
The distance between the lamps and the surface of baby was kept constant
at 45 cm. The irradiance of the phototherapy unit was measured every 8 h
at level of skin of abdomen of the neonate using a standard flux meter
(Ginevri, Rome, Italy) sensitive to wavelengths of 425-475 nm.
Outcome measurement: During phototherapy,
STB was measured every 8-12 h. Venous blood samples were obtained in
pre-heparinized capillaries, spun and analyzed with a twin-beam
spectrophotometer (Ginevri, Rome, Italy). Mother’s and neonates’ blood
group and Rh type, peripheral smear for hemolysis, reticulocyte count,
direct Coomb’s Test and G6PD status were determined. If phototherapy was
started after 72 h of age, it was discontinued if two consecutive STB
levels measured 8-12 h apart, were less than 15 mg/dL. If phototherapy was
started before 72 h of age, it was discontinued when two consecutive STB
values measured 8-12 h apart, were less than the age-specific threshold
for initiating phototherapy. Rebound of jaundice was clinically evaluated
8 hours after stopping phototherapy. A single unit phototherapy was said
to have ‘failed’ if at any time during phototherapy a STB of >20 mg% was
documented. Such a baby was treated with intense phototherapy with 2
conventional units or a conventional unit and a fibreoptic bed
phototherapy, based on the availability. All neonates wore eye pads and
diapers while under phototherapy. Rooming-in and exclusive breast feeding
were encouraged. Mother was allowed to switch-off the lights during
nursing and diaper change. Neonate’s temperature was monitored every 6 h.
Side effects like loose stools, feed intolerance, skin rashes were
recorded. Duration of phototherapy was calculated from the inbuilt hour
counter.
Sample size and statistical analysis: Based on a
previous study(9), average duration of phototherapy required in term
neonates with non-hemolytic jaundice using a single unit phototherapy is
39.0±14.7 h. For detecting 20% difference in duration of phototherapy with
two-sided alpha of 0.05 and 90% power, 75 subjects were needed to be
enrolled in each group. Data were entered and analyzed using Epi Info™
Version 3.3.2 (CDC, Atlanta, US). Chi square and two-sample t-test
were used for discrete and continuous variables respectively. Analysis was
based on intention-to-treat.
The study was approved by the Institutional Ethics
Committee and written informed consent was obtained from one or both
parents prior to enrollment.
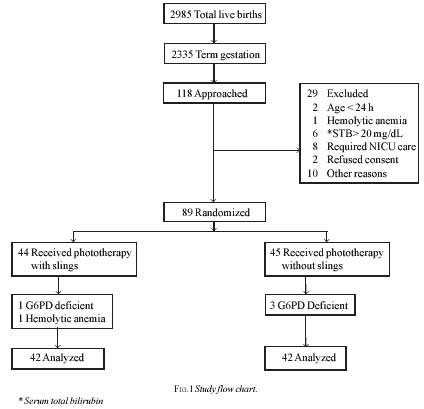
Results
Fig.1 details the flow of participants in the
trial. One baby in the Sling group and three in the No sling group were
detected to have G6PD deficiency after enrollment. Another neonate
enrolled in the Sling group was found to have hemolysis of uncertain
etiology. Infants with G6PD deficiency and hemolysis were not included in
analysis.
The Sling and No sling groups were comparable with
respect to birth weight, gestational age, gender and other maternal and
neonatal variables (Table I). However, diabetes mellitus was
more frequent in the mothers of babies in the No sling group. Age at onset
of phototherapy, initial STB and packed cell volume (PCV) were also
similar in two groups. Phototherapy units in Sling group had a
significantly higher flux (Table I).
Table I
Demographic and baseline variables
Demographic data
|
Sling group
(n=42) |
No Sling
(n=42) |
| Males |
25 (60%) |
22 (52%) |
| Gestational age (wks) |
38 ±1.3 |
37±1.0 |
| Birth weight (g) |
2790±351 |
2923±330 |
| Vaginal delivery |
29(69%) |
24 (57%) |
| Caesarean section |
5(12%) |
9(21%) |
| Forceps delivery |
6(14%) |
1(3%) |
| Vacuum |
2(5%) |
8(19%) |
| Oxytocin to mother |
32(72%) |
27(64%) |
| Diabetes mellitus |
10(24%) |
3(7%) |
| Hypertension |
6(14%) |
4(9.5%) |
| Hypothyroid |
3(7%) |
1(2.4%) |
| Small-for-gestation |
1(2) |
0 |
| Large-for-gestation |
1(2) |
3(7) |
| Minor internal bleed |
0 |
1(2.3%) |
| 5 min Apgar (range)* |
8-9 |
8-9 |
| ABO incompatibility setting |
13(32%) |
12(29%) |
| Rh Negative neonates |
0 /21 (0%) |
3/23 (13%) |
| Rh Negative mothers |
2/41(4.9%) |
2/41(4.9%) |
| Variables at start of phototherapy |
| *Age (h) |
65 ±24.9 |
73±44 |
| *Total serum bilirubin (mg/dL) |
16.6±2.4 |
16.1±2.2 |
| *Packed cell volume (%) |
52±5.7 |
51±5.6 |
| #Flux (microwatt/cm2) |
194.1±26 |
179.7±27.7 |
All values except * expressed in number (%) or mean ±SD
* P>0.05; # P= 0.01
Outcome variables for the two groups are compared in
Table II. None of neonates in either group required exchange
transfusion. There was no significant difference in STB at start of
phototherapy, postnatal age at start of phototherapy, ABO incompatibility
setting, G6PD deficiency and minor internal bleed in the neonates who
failed single-surface phototherapy and those who did not. None of the
participants developed hyperthermia, feed intolerance, vomiting, decreased
urine output, and skin rashes.
Table II
Primary and Secondary Outcomes
| Outcome |
Sling group (n=42) |
No sling group (n=42) |
P value |
| Duration of phototherapy (h) |
23.3±12.9 |
24.9±15.4 |
0.6 |
| Mean difference (95% CI) |
–1.67 (–8.00 to 4.66) |
|
|
| #Failure of single surface phototherapy* (n, %) |
4 (9.5%) |
5(12%) |
0.5 |
| #TSB at the end of 8 h (mg/dL) |
15±3.3 |
16±2.9 |
0.19 |
| #TSB at cessation of phototherapy (mg/dL) |
12±1.8 |
12±1.6 |
0.37 |
| +Rate of fall of TSB in first 8 h (mg/dL/h) |
0.23±0.49 |
0.03±0.47 |
0.06 |
| #Absolute fall of TSB in first 24 h (mg/dL) |
2.3±3.3 |
2±3.7 |
0.65 |
| #Percent fall of TSB in first 24 h (%) |
19.5+23.0 |
13.5±10.9 |
0.57 |
All values except * in mean ±SD; #P>0.05; +P=0.01; h=hours, TSB = Total serum bilirubin.
Discussion
Our study investigated the use of slings made of white
reflective material in increasing efficacy of a single-surface CFL
phototherapy. We did not observe any significant difference in mean
duration of phototherapy on addition of slings to phototherapy units,
although the irradiance of phototherapy unit in Sling group was marginally
higher. The rate of fall of STB in first eight hours showed a trend
towards being higher in the study group.
Djokomuljanto, et al.(7) and Hansen, et al.(8)
have reported significant increase in irradiance and shortening in the
duration of phototherapy on using slings. Djokomuljanto, et al.(7)
used locally produced underpads (used to protect the sheets of the cots
against faecal or urinary soiling) as slings and Hansen, et al.(8)
used white bed sheets around cots. Although, previous investigators
have employed different thresholds for initiation or discontinuation of
phototherapy, use of different guidelines should not interfere with the
comparison of various studies if same cut-offs are used in experimental
and control groups.
With standard phototherapy systems, a decrease of 6% to
20% of the initial bilirubin level can be expected in the first 24
hours(10) and we documented a comparable 19.5+23.0% (mean+SD)
decline in the Sling and 13.5+10.9% decline in the No sling group.
Our inability to find any significant difference in duration of
phototherapy may be due to lower reflective index of the sling material,
lower initial STB, varying level of production of bilirubin or other
unknown factors. The fourth side of the phototherapy unit was without any
sling in the Sling group. This could have lessened the potential efficacy
of sling application.
Neonates with hemolytic jaundice were excluded from our
study, because they have more rapidly rising and higher initial STB and
are more likely to need intensive phototherapy or exchange transfusion.
Therefore, use of ‘sling-enhanced’ phototherapy in them needs to be
investigated separately. Our study included only term babies, because the
guidelines for preterm babies are different and the premature babies are
more susceptible to bilirubin-induced neurotoxicity because of the
immaturity of the blood brain barrier and other co-morbid conditions.
We monitored babies for hyperthermia, hypothermia, feed
intolerance, skin rashes and did not find any in either group. The slings
did not interfere with the monitoring and nursing the babies. They may
have affected the mother – infant bonding and caused eyestrain to health
care workers. These side effects were not monitored. The feeding patterns
and postnatal weight loss of babies were also not monitored.
The present study has few limitations. We estimated the
total bilirubin for monitoring the response to phototherapy. The
predominant process of bilirubin elimination by phototherapy, and probably
the rate-limiting mechanism, is the irreversible photo-alteration of
bilirubin to a structural isomer called lumirubin, which is not separately
measured by spectrophotometers. Chromatographic methods to measure
lumirubin levels although not routinely available would have been a better
indicator of efficacy of sling phototherapy. Since the retrospectively
calculated power of the study is only 18%, the study may be underpowered
to find a difference in duration of phototherapy between the two groups.
The strengths of the present study are its design, minimal trial deviates
and accurate measurement of duration of phototherapy.
In conclusion, reflective slings in CFL phototherapy
units as used in our study resulted in a marginal increase in irradiance
and a trend towards a greater rate of fall in total serum bilirubin in
term neonates with non-hemolytic settings. However, there was no reduction
in duration of phototherapy with use of this intervention.
Contributors: SS participated in acquisition of
data and manuscript preparation, DC participated in analysis,
interpretation of data and manuscript preparation, SM participated in
acquisition of data, RM participated in study design and manuscript
preparation, AKD participated in concept, design and critical review.
Funding: None.
Competing interest: None stated.
|
What is Already Known?
• Efficacy of phototherapy can be increased by
increasing surface area of exposure and by increasing the
irradiance.
What This Study Adds?
• Addition of white reflective slings increased the irradiance of
compact fluorescent light phototherapy. |
References
1. Vreman HJ, Wong RJ, Stevenson DK. Phototherapy:
current methods and future directions. Semin Perinatol 2004 ; 28: 326-333.
2. American Academy of Pediatrics, Subcommittee on
Hyperbilirubinemia. Management of hyperbilirubinemia in the newborn infant
35 or more weeks of gestation. Pediatrics 2004; 114: 297-316.
3. Dicken P, Grant LJ, Jones S. An evaluation of the
characteristics and performance of neonatal phototherapy equipment.
Physiol Meas 2000; 21: 493-503.
4. Maisels J M. Why use homeopathic doses of
phototherapy? Pediatrics 1996; 98: 283-287.
5. Tan KL. Efficacy of bidirectional fiber-optic
phototherapy for neonatal hyperbilirubinemia. Pediatrics 1997; 99: e13.
6. De Carvalho M, De Carvalho D, Trzmielina S, Lopes
JMA, Hansen TWR. Intensified phototherapy using daylight fluorescent
lamps. Acta Pediatr; 88: 768-771.
7. Meslo MTL, Hansen TWR. Effektivisering av
lysbehandling med enkle midler. Jordmorbladet 2000; 7: 18-21.
8. Djokomuljanto S , Qua BS, Surini Y, Noraida R ,
Ismail NZN, Hansen TWR, et al. Efficacy of phototherapy for
neonatal jaundice is increased by the use of low-cost white reflecting
curtains. Arch Dis Child Fetal Neonatal Ed 2006; 91; F439-442.
9. Sarici SU, Alpay F, Unay B, Ozcan O, Gokcay E.
Double versus single phototherapy in term newborns with significant
hyperbilirubinemia. J Trop Pediatr 2000; 46: 36-39.
10. Tan KL. Comparison of the efficacy of fibreoptic
and conventional phototherapy for neonatal hyperbilirubinemia. J
Pediatr1994; 125: 607-612.
11. Fiberoptic phototherapy systems. Health Devices
1995; 24: 132-153.
12. Sarici SU, Alpay F, Dundaroz MR, Ozcan O, Gokcay E.
Fibreoptic phototherapy versus conventional daylight phototherapy for
hyperbilirubinemia of term newborns. Turk J Pediatr 2001; 43: 280-285.
13. Garg AK, Prasad RS, Hifzi IA. A controlled trial of high-intensity
double-surface phototherapy on a fluid bed versus conventional photo-
therapy in neonatal jaundice. Pediatrics 1995; 95: 914-916. |
|
|
 |
|