|
|
Case Reports Indian Pediatrics 2008;45:58-60 |
||||
|
Pneumoparotitis with Subcutaneous Emphysema |
||||
|
S Balasubramanian From the Pediatric Rheumatology Clinic, Jaslok Hospital & Research Center, Mumbai 400 016.
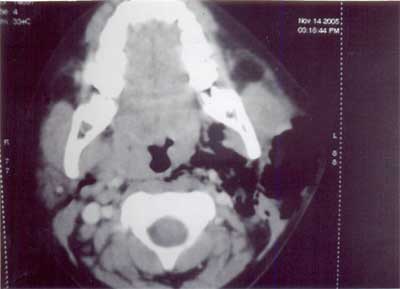
Abstract: Pneumoparotitis refers to air within the parotid gland with or without inflammation. Self-induced pneumoparotitis is a very rare entity in children. We describe self-induced pneumoparotitis in an adolescent boy where we could identify the diagnosis only after extensive investigations. Case Report An 11-year old boy presented with recurrent swelling of the parotid glands for 2 years. Despite multiple courses of antibiotics, the swellings continued to appear, each time lasting for about 4-5 days, never associated with upper respiratory tract infections or fever and characterized by spontaneous resolution. On inspection, he was a cheerful and plump boy who had enlargement of his left parotid gland with purulent discharge from the Stenson’s duct. In addition he had crepitus over the submandibular area indicating the presence of subcutaneous emphysema. His blood counts and acute phase reactants were within normal limits and culture from the Stenson’s duct did not grow any organism. He tested negative for HIV serology and imaging of the parotid gland revealed emphysematous changes (Fig. 1). A radionuclide sialogram was performed which showed evidence of reduced function in the left parotid gland. Biopsy of the parotid gland showed aggregates of numerous multinucleated foreign body type giant cells. After extensive investigations to rule out Sjogren’s syndrome, sarcoidosis and immunodeficiency states, he was labeled as having juvenile recurrent parotitis and advised mouthwashes, local massages along with daily oral penicillin.
He came back a month later with increasing swelling and subcutaneous emphysema extending up to his eyelids (Fig. 2). His apparent lack of concern towards his own ailment, the facial disfigurement it caused and the loss of school days along with the mysterious exacerbations and remissions prompted us to think of an underlying psychological problem. A detailed psychological evaluation revealed sibling rivalry with his 3-year old sister. The parents reported that the boy used to frequently stand in front of the mirror with a handkerchief in his hand and blow forcefully into his closed hand puffing out his cheeks. This Valsalva like maneuver was probably causing pneumo-insufflation of the parotid gland. With adequate counseling, the boy made a dramatic recovery with reduction in the size of the swelling and complete disappearance of subcutaneous emphysema.
Discussion The pneumatic enlargement of the parotid gland is caused by air insufflation via the Stenson’s duct orifice into the more proximal ductal system and gland. The contracted buccinator muscle usually compresses the parotid duct and increases the duct angulation thus preventing air insufflation during surges in intra-oral pressure. The small diameter and slit like shape of the duct orifice covered by mucous membrane folds are additional natural protective mechanisms that prevent air insufflation(1). Pneumoparotitis is thus seen in conditions with a supra normal increase in intra-oral pressures; as in players of wind instruments and glass blowers (up to 140-150 mmHg). A similar inflated-cheek increase in oral pressure probably lies behind the reported cases of non-occupational pneumoparotitis, which seem correlated with two aspects i.e., adolescent age group and their psychological behavior. The reported abnormalities in the psychological background of adolescents with pneumoparotitis are conflicts with parents, nervous tics, adolescent adjustment reactions, abnormal behavior and previous psychiatric treatment(2). In our case, pneumoparotitis was a manifestation of an adjustment reaction to adolescence precipitated by sibling rivalry. Recurrent parotid insufflation is not entirely benign and may predispose to sialectasis, recurrent parotitis and even subcutaneous emphysema of the face, neck and mediastinum and subsequent pneumothorax(3). Superimposed bacterial infection due to salivary retention within the ectatic ducts can complicate pneumoparotitis, which can be bilateral, and the diagnosis is difficult in such cases, often made only after exclusion of obstructive, inflammatory and neoplastic causes of parotid enlargement including an anerobic infection of the parotids(4,5). Pneumoparotitis has also been described following orthodontic procedures and general anesthesia(6). Treatment is reassurance and elimination of the precipitating maneuver. Prophylactic antibiotics directed towards Pneumococcus, Staphylococcus and H. influenza have been used by some clinicians because of the fear that refluxed oral bacteria may produce an acute suppurative parotitis(3). Though benign recurrent parotitis has been reported in Indian literature(7,8), this is the first report of pneumoparotitis in Indian literature. The presence of la belle indifference and prolonged school absenteeism in an adolescent should alert us to search for a psychological cause for pneumoparotitis. Contributors: All authors contributed to writing, collating and managing this case. Funding: Nil. Competing interests: None stated. | ||||
|
References | ||||
|
![]()