|
|
Research Paper Indian Pediatrics 2008; 45:17-23 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Kangaroo Mother Care for Low Birth Weight Infants: A Randomized Controlled Trial |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
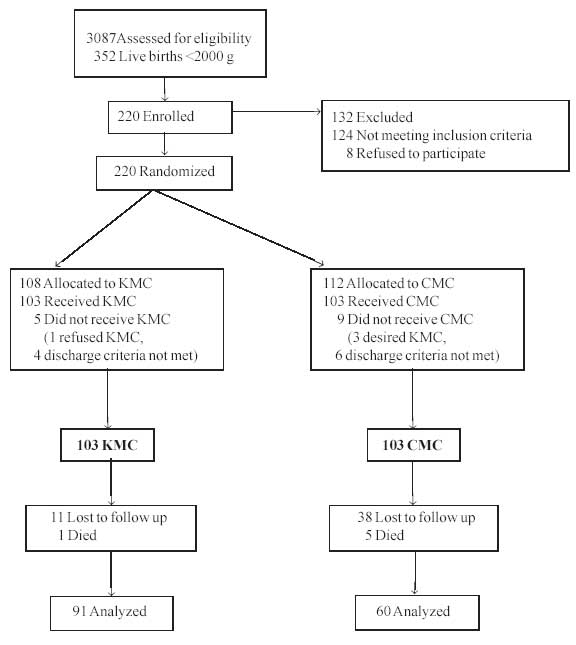
Introduction Kangaroo mother care (KMC) is a humane, low cost method of care of low birth weight (LBW) infants particularly for those weighing less than 2000 g at birth. It consists of skin-to-skin contact, exclusive breastfeeding and early discharge with an adequate follow-up(1,2). Knowledge on the effectiveness and safety of KMC in the community/home settings and its effects on growth is still incomplete(3). Despite the said advantages of KMC, it is still not a widely practiced method of care of LBW infants in India(4); also, there is insufficient data regarding the effect of KMC on growth parameters, acceptability of kangaroo care and long-term outcomes. We conducted this study to assess the effect of KMC on growth of infants weighing <2000 g at birth. Methods This prospective randomized controlled trial was conducted in a teaching institution with a tertiary level neonatal intensive care unit (NICU) in Western India over a 9 month period. The study population included 206 consecutive singleton intramural neonates with birth weight <2000 g. Critically ill babies requiring ventilatory or inotropic support, babies with chromosomal and life threatening congenital anomalies, babies requiring transfer, or whose mothers were critically ill, or unable to comply with the follow up schedule were excluded. The sample size was calculated to achieve a power of 80% and a error of 0.05, based on an earlier study by Hann et al.(5). The primary outcome variable was "weight gain". Secondary measures included neonatal morbidity, mortality and duration of hospitalization. We also studied whether KMC was acceptable by the mother at home. The subjects were randomized into two groups: Kangaroo Mother Care (KMC) and Conventional Method Care (CMC). Randomization was achieved by simple randomization and allocation was concealed by sealed envelope technique. KMC group: Mothers in the KMC group were explained in detail about KMC adoption in the presence of their family. KMC was initiated as soon as the baby was stable. The mothers provided skin to skin contact using a specially tailored "Kangaroo bag" made of soft flannel cloth. The mothers were encouraged to keep the baby in KMC as long as possible during the day and night with a minimum period of one to two hours at a time. When the baby was receiving intravenous fluids, mother provided kangaroo care seated in a comfortable chair placed close to the baby’s cradle. Once the baby was on full feeds, she provided kangaroo care on the reclining cot in the semi-upright position with the help of pillows. When the baby was not in KMC, the baby was placed either under a servo controlled radiant warmer or in the cradle under hot lamp adequately clothed and covered. The mothers were given a "KMC chart" to keep a record of the duration of kangaroo care provided. If the mother was unable to fill up the chart, it was done by a close family member. CMC group: The babies assigned to CMC group were managed under either servo controlled radiant warmers or in a cradle under hot lamps in NICU. The babies in postnatal wards were adequately clothed and bedded in with their mothers. Anthropometry: Babies were weighed naked on an electronic weighing scale (Conweigh Electronic weighing scale - accuracy of ± 5 g) immediately after birth and subsequently daily one hour after feeds till discharge. The weighing machines were calibrated daily with 5 g standard weight. The length was measured at birth, on discharge and on each follow-up visit by using an infantometer. Head circumference (HC), chest circumference (CC), mid-arm circumference (MAC) and foot length were measured by standard methods at birth, on discharge and on each follow-up visit with a non-stretchable tape. All measurements were carried out by the same clinician. Feeding: All babies were exclusively breastfed, and also received calcium (100 mg/kg/d), phosphorus (50 mg/kg/d) and multivitamin supplements. Babies unable to take direct breastfeeds were given expressed breast milk by orogastric tube or using a bondla or sterile wati and spoon. Monitoring: Babies in both the groups were monitored for hypothermia, hypoglycemia, apnea, sepsis, feeding problem and other morbidities. Babies who developed a life threatening event like convulsions, hypothermia, severe sepsis were considered as critically ill and were temporarily withdrawn from the KMC group. Babies requiring phototherapy were also temporarily withdrawn from KMC group. Discharge and follow up: Babies were discharged when they showed a weight gain of 10-15 g/kg/d for three consecutive days, were feeding well, maintaining temperature without assistance and the mother was confident of caring for her baby. They were followed up weekly for anthropometry and compliance with KMC, in the high risk OPD till post-menstrual age of 40 weeks in preterm babies or till a weight of 2500 g was reached in term SGA babies. Mothers in the KMC group were interviewed on a pre-structured questionnaire to assess the acceptability and feasibility of KMC in the hospital and at home. Statistical analysis: Data were recorded on a pre-designed proforma, tabulated and the results were analyzed statistically by SPSS statistical software (version 10.1). Pearson’s Chi-square test was used to test the association of columns and rows in tabular data, in case of qualitative, categorical data. Student’s t-test and Analysis of variance was used to compare quantitative measurements. A P-value of <0.05 was considered significant. Ethics: The approval from the Institutional Ethics Committee was obtained prior to the study. A written informed consent was taken from the mothers after the babies were stable and ready for enrolment into the study. Results Figure 1 depicts the study enrolment in detail. The final study groups comprised of 103 KMC babies and 103 CMC babies. Their baseline characteristics are compared in Table I. The mean birth weight and gestational age of the KMC group was lower than that of the CMC group. Almost 70% of babies from the KMC group received NICU care as compared to 57.3% of CMC babies (P = 0.06). Table I Neonatal Baseline Characteristics
KMC - Kangaroo mother care;
CMC - Conventional method of care. Figures in parentheses indicate percentages.
Effect on growth: KMC babies achieved significantly better growth at the end of the study (Table II). For preterm babies, weight, length and head circumference were significantly higher in the KMC group (weight 2388 g, length 47.8 cm and head circumference 33.4 cm) than in the CMC group (weight 2065 g, length 46.4 cm and head circumference 32.1 cm) at the end of follow-up (P <0.05) . Table II Effect of KMC on Growth (at 40 Weeks Postmenstrual Age in Preterm Babies and After Attainment of 2500 g in Term SGA Babies)
Morbidities: A significantly higher number of babies in the CMC group suffered from hypothermia, hypoglycemia, nosocomial sepsis, compared to the KMC group. KMC significantly reduced the incidence of apnea in VLBW babies. More CMC babies were not on exclusive breastfeeds at the end of the study (76% vs 98%). The time taken to reach full feeds and the time to reach initiation of direct breastfeeds were comparable in both the groups (Table III). One baby in the KMC group and 5 in the CMC group died during the study (RR 5, 95% CI 0.59 to 42.06). Table III Effect of KMC on Morbidities
KMC - Kangaroo mother care; CMC - Conventional method of care
Acceptability of KMC: KMC was acceptable to most mothers and families. A majority of mothers expressed happiness (71.5%), practiced KMC easily (75.5%), without assistance (80.39%) and felt that their baby preferred KMC (65%). The KMC babies received kangaroo care for a mean of 33.78 ±15.12 days at 13.5 hours per day. A few mothers provided almost 24 hours at home. Discussion The goal of nutritional management of the LBW infants is the achievement of postnatal growth at intra-uterine growth accretion rates(6). We demonstrated a significantly higher daily weight gain in infants who received the KMC intervention. This beneficial effect was reflected in other growth parameters and is comparable with other studies (5,7,8). The recommended weekly increment of 0.75 cm in head circumference was achieved only in the KMC group(9). Head circumference has been emphasized to be one of the most important growth parameters in LBW babies(10,11) being a reflection of the underlying brain growth. Kangaroo care by promoting exclusive breastfeeding, ensuring temperature maintenance, facilitating physiologic stability and decreasing neonatal morbidities, could result in improved physical and cognitive growth (12). However, the weight of preterm babies at 40 weeks postmenstrual age was lower than the average birth weight of normal full term Indian babies even in the KMC group and lower than that documented in other studies(13). The lack of use of formula feeds, fortifiers and shorter duration of Kangaroo care compared with other studies could have resulted in poorer weight gain(13). Our study confirms previous findings of the definite protective effect of KMC against hypo-thermia, hypoglycemia, apnea and sepsis. However, we did not observe a difference in the duration of hospitalization between the two groups. In our unit, discharge criteria for low birth weight babies is weight gain of at least 10 g/kg/d for 3 consecutive days, irrespective of the actual weight or gestation of the baby. If we had used fixed target weight criteria for discharge as in other studies(7), it is likely that the KMC group would have shorter hospital stay considering their higher daily weight gain. In the present study, the mean duration of KMC provided was 13.5 hours per day. The shorter duration of skin-to-skin-contact in the present study in comparison to other studies(8,10,13) could be due to the promotion of the mother alone as the kangaroo care provider due to the institutional policies preventing the father and the relatives to be with the baby in the NICU or postnatal wards. The other studies involved the father or other close relatives in kangaroo care. However, the average maximum duration per day of 19 hours achieved by the mothers in the KMC group and the success of a few mothers to provide almost 24 hours per day kangaroo care suggested that with further motivation, education and involvement of the family, 24 hours kangaroo care in the home settings is definitely feasible. One of the strengths of our study is the high follow-up rate among KMC infants, comparable to other studies(13). The better follow-up rate in the KMC group could be due to the active involvement of the mother in the care of her LBW baby or the strong rapport between the KMC mother and the health personnel. The poor follow-up in the CMC group is a limitation of this study. Home visit was not possible in the present study. However, the higher follow-up by KMC mothers suggests that early discharge with regular follow-up of LBW infants is definitely feasible without compromising on the health of the baby. In the present study, maternal acceptance of KMC was good and concurred with other studies(7,8,14). All the mothers were able to practice KMC at home and no adverse events were reported. The response of the family and/or the father was supportive. One third of the mothers were confident enough to serve as advocates for KMC during hospital stay and they were an important source of support for the newly enrolled mothers. This study has demonstrated that KMC is feasible in the Indian household. However, KMC was initiated in the hospital under close supervision and guidance and only later continued at home. Further research should investigate the implementation of KMC after initiation in the community. We conclude that KMC improves growth in low birth weight infants and has a significant role in protecting the LBW infant from hypothermia, hypoglycemia and sepsis. We recommend Kangaroo care for low birth weight infants. It is definitely feasible, acceptable to mothers and can be continued at home in the Indian set up. Contributors: SRPN: Concept, design, acquisition of data, analysis, interpretation and writing of manuscript; RU: Concept, design, analysis and critical revision of manuscript; and RN: Conception, design, analysis and critical revision of manuscript. Source of funding: None. Competing interest: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()