|
|
Correspondence Indian Pediatrics 2007; 44:51-52 |
|||||
|
A Technique of Transporting Neonates with Gastroschisis |
|||||
|
Prior to 2003 our results were also very poor. On clinical audit, we recognized that it is the faulty referral which is responsible for poor outcome in many cases. These neonates were used to be referred with the intestines wrapped in sterile gauze pads or cotton wool. These dressing materials, although sterile initially, quickly become unsterile when being soaked with peritoneal exudates. Such wet fabrics are ineffective in preventing bacterial contamination because microbial ingress occurs by capillary action. Wet gauze dressing also promotes evaporative loss thereby inducing hypothermia and dehydration. Moreover, the minute lint shed from these materials are difficult to get rid of and they act as nidus of postoperative infection. In 2003 we devised a protocal and circulated it to all the local medical practitioners of our area.
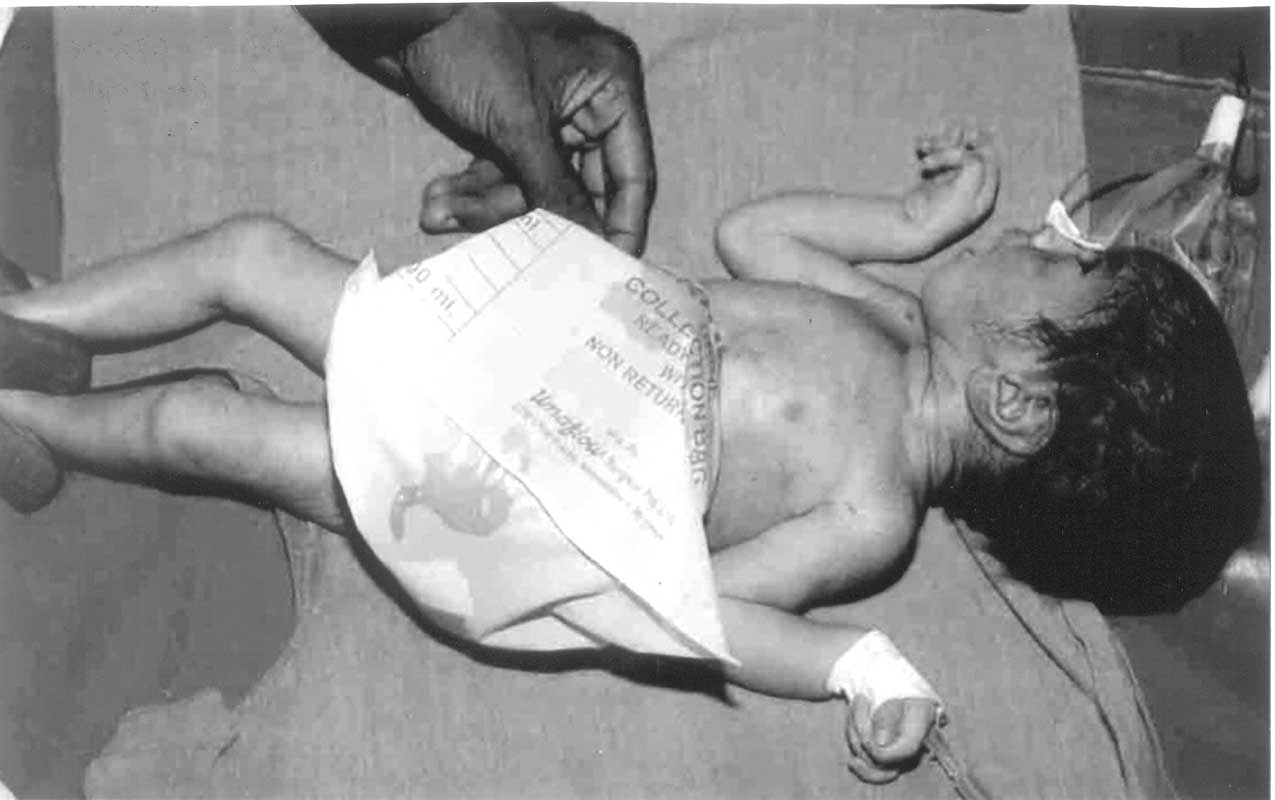
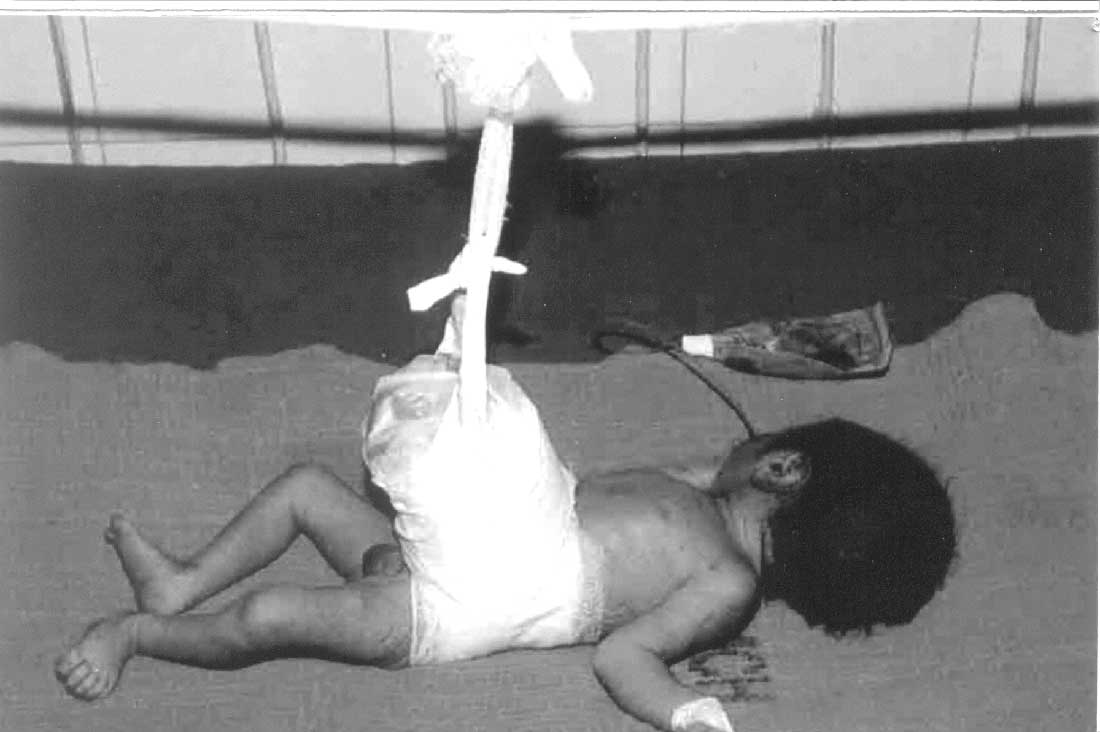
According to this protocol, the referring pediatrician is encouraged to gently wash the exposed intestine with lukewarm sterile normal saline. This will decontaminate microbes that were acquired during vaginal delivery. The bowel loops are then placed inside a cut-open sterile Urobag™ (urine-collecting bag) (Fig.1). Outer to the plastic bag, a layer of sterile absorbent gauze packs are kept and bandaged. This bag is vertically suspended to prevent kinking of bowel (Fig.2). This is important because kinking may lead to ischemia and gangrene. As the plastic bag is impervious, evaporative heat loss and dehydration are prevented. The transparent bag also permits frequent inspection of the viability of the bowel loops during transport without disturbing the dressing. Urobag™ is easily available and is economically cheap.
Survival in the last two years approached 75% as compared to 5% in the pre-campaign year. Even we have recently set the Indian record of the survival of the lowest weighing gastroschisis baby(4). Improved quality of nursing care is also partly responsible for the reduced mortality, besides proper referral and transport. V. Raveenthiran,
|
![]()