|
|
Lead Article Indian Pediatrics 2007; 44:15-24 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Effect of Iron Supplementation on Physical Performance in Children and Adolescents: Systematic Review of Randomized Controlled Trials |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
#Sunder Lal Jain Hospital, New Delhi 110 052, India; *Sitaram Bhartia Institute of Science and Research, B-16 Qutab Institutional Area, New Delhi 110 016; **HarvestPlus, International Food Policy Research Institute, 2033 K Street, NW, Washington, DC 20006-1002, USA.
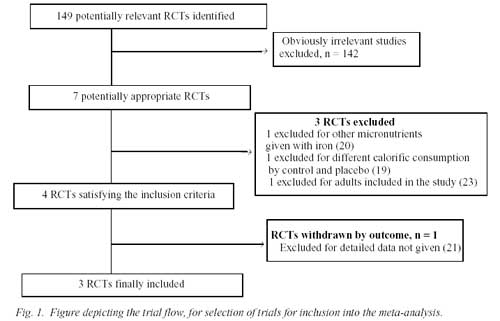
According to the estimates of the World Health Organization (WHO), more than one third of the world’s population is anemic; nearly two billion individuals are affected(1). Recent estimates from India documented an anemia prevalence of 74% in children between 9 to 36 months of age(2). Amongst the various causes of anemia, iron deficiency is believed to be of foremost importance(3). Observational studies in humans have documented a relationship between iron deficiency anemia and impaired physical performance(4,5). According to estimates, each 1% drop in hemoglobin results in 1.5-2% decrease in work capacity and output(6). However, the findings from intervention trials are not consistent regarding the role of iron supplementation in improving the physical performance. Increase in hemoglobin has been shown to result in improved work tolerance(7). Other data suggests that raising the serum ferritin levels has no impact on the maximal work capacity(8). Another interesting dimension has been added to the controversy by the possible contributions of vitamin B12 and folate to anemia and impaired physical performance. In view of the conflicting evidence available, we conducted a systematic review to evaluate the effect of iron supplementation on physical performance in children and adolescents. Subjects and Methods Search Strategy We searched computerised bibliographic medical databases till March 2003, including Medline (data available from 1966), Cochrane controlled trials register, Embase, International Bibliographic Information on Dietary Supplements Database (IBIDS), and Healthstar for trials in English language. We also reviewed reference lists of identified articles and hand searched reviews, bibliographies of books, and abstracts and proceedings of international conferences or meetings. Donor agencies, "experts", and authors of recent iron supplementation trials were contacted to identify any additional or ongoing trials. The title and abstract of the trials identified in the computerised search were scanned to exclude studies that were obviously irrelevant. We reviewed the full texts of the remaining studies and identified trials that fulfilled the inclusion criteria. To avoid publication bias, we included published and unpublished trials. Selection criteria Randomized placebo controlled trials investigating the effect of oral iron supplementation/ iron fortified milk or cereals on physical performance (as assessed by heart rate, treadmill endurance time, blood lactate levels or oxygen consumption) in children and adolescents were included. Non-placebo controlled trials were considered only if the iron was given parenterally. We also included studies in which other micronutrients and drugs were simultaneously administered if the only difference between the study and the control groups was iron supplementation. Validity assessment We assessed the quality of trials using recommended criteria(9,10). Concealment of allocation was classed as adequate, unclear, inadequate, or not used (labelled as A,B,C and D, respectively). To assess attrition we classified studies by percentage of participants lost to follow up (A: <3%, B: 3-9.9%, C: 10-19.9%, and D: >20%). Blinding was classified as double blinding (A), single blinding (B), no blinding (C), and unclear (D). Data abstraction Preformed questionnaires were used to abstract data. The data included in this review were derived from the published papers or were provided by the authors. If required, and wherever possible, we contacted the authors for clarifications. Quantitative Data Synthesis In studies with two or more iron intervention groups (different dosage or administration regimes) and a single control group, the sample size of the control group was divided equally between the number of intervention groups while retaining the same value for the change in outcome and its standard deviation (SD). This was done to avoid multiple counting of the control group (Oxman AD, Personal Communication, 2003; Deeks J, Personal Communication, 2003). Thus, some trials contributed more than one analytic component for statistical computations. In computing pooled estimates, we required sample size, mean change in development score from the beginning to the end of the intervention, and the SDs of this change in the intervention and control groups. The following principles were used for derivations if actual variables were not stated: (i) in a group the lower of the two stated sample sizes at the beginning or at the end of a trial was assumed to be the sample size for the change; (ii) wherever feasible, SDs were back calculated from the stated standard errors, t, or p values; (iii) wherever not stated, the mean change in development score was computed as the difference of mean post- and pre-intervention scores; and (iv) wherever not stated, the mean age of subjects was computed as the average of the stated range. The SD for the change in development scores was computed assuming correlations of 0.5, and 0 (independent) between the pre- and post-test variances(11). The presence of publication bias, that refers to the greater likelihood of research with statistically significant results to be submitted and published compared with non-significant or ‘null’ results, in the extracted data was evaluated by funnel plots(12). We used the metabias command in STATA software to perform statistical tests for funnel plot asymmetry(13). The pooled estimates of the weighted mean difference (WMD) of the evaluated change in outcome score between the control and intervention group were calculated by both fixed effects and random effects model assumptions using the "metan" command in STATA software(13). We report primarily random effects estimates because most of the pooled results obtained were statistically heterogeneous. In view of the limited number of studies available, stratified analyses and metaregression were not done. Results A total of 7 studies(14-20) were identified to be potentially eligible for inclusion in the systematic review. After thorough scrutiny, 3 trials were included (Fig. 1).
Table I depicts the baseline characteristics of the analyzed trials. TABLE I Baseline Characterstics of the Included Studies
The parameters to assess physical performance were different in the three studies. Gopaldas, et al.(15) estimated the effect of iron supplementation on submaximal work capacity (using the modified Harvard Step Test) by estimating the heart rates and the blood lactate levels after exercise. Powers, et al.(14) studied the effect of iron therapy on running performance, on a treadmill at three different speeds (5,6 and 7 miles per hour), by evaluating the heart rate and oxygen consumption. Rowland, et al.(19) measured treadmill endurance time, heart rate and submaximal and maximal oxygen consumption. Heart rates measured after exercise in the three studies were considered to be ‘combinable’ for the purpose of meta- analyses. The other parameters are discussed individually. Heart rate Three studies were included in this meta-analysis. Amongst these, Powers, et al.(14) evaluated the effect of iron supplementation on heart rate, at three different running speeds.
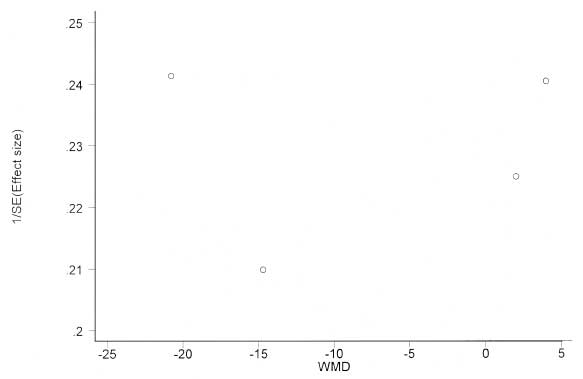
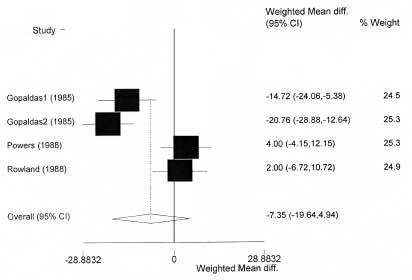
Pooled results with running performance at 5 mph: There was no evidence of bias on funnel plot (Fig. 2) or by using the Egger’s (weighted regression) method (p for bias = 0.91) or the Begg’s (rank correlation) method (continuity corrected p = 1.00). Pooled data was available for 106 children, 61 of whom received iron while 45 constituted the placebo group. The pooled weighted mean difference (WMD) in the heart rates between the iron and the placebo, following exercise, in the 4 analytic components was –7.3/ min (95% CI = –19.6, 4.9, p = 0.24; test for heterogeneity = 24.72, p<0.001) (Table II and Fig. 3).
Pooled results with running performance at 6 mph: There was no evidence of publication bias. The pooled WMD in the heart rates between the iron and the placebo, following exercise, with assumption p = 0.5, in the 4 analytic components was –6.6 /min (95% CI = –19.9, 6.6; p = 0.33; test for heterogeneity = 28.13, p <0.001) (Table II). TABLE II Pooled Change in Post-exercise Heart Rate
Pooled results with running performance at 7 mph: There was no evidence of publication bias. The pooled WMD in the heart rates between the iron and the placebo, following exercise, with assumption p = 0.5, in the 4 analytic components was –8.0/min (95% CI = –19.7, 3.7; p = 0.18; test for heterogeneity = 20.65, p <0.001) (Table II). Blood lactate Blood lactate levels before and after exercise was estimated in one study only(15). The lactate levels in those supplemented with either 30mg or 40mg of elemental iron were significantly lower (p <0.05) than that of the placebo both before (7.71 and 7.55 mg/dL versus 8.43 mg/dL) and after (14.36 and 14.35 mg/dL versus 16.48 mg/dL) exercise, following iron supplementation. The authors further divided the study cohort into anemic and non-anemic children. The non-anemic subjects had significantly lower (p <0.05) blood lactate levels compared to their anemic counterparts in the pre-supplementation period. After iron supplementation, the lactate level of the non-treated anemic subjects was higher than the iron supplemented group, both pre and post-exercise (p <0.05). In the pre-exercise stage, non-anemic subjects had significantly lower (p <0.05) lactate levels than the anemic group. After exercise, the group receiving 40 mg iron had significantly lower (p <0.05) lactate levels when compared with the placebo group, but there was no difference in the lactate levels between the group receiving 30 mg iron and placebo. Oxygen consumption Oxygen consumption was estimated in two studies. Powers, et al.(14) showed a significant increase in oxygen consumption in both the placebo and the iron treated group following supplementation at all three running speeds: 5 mph (0.06 L/min for placebo and 0.03 for iron group), 6 mph (0.1 L/min for placebo and 0.07 L/min for iron group) and 7 mph (0.13 L/min for placebo and 0.11 L/min for iron group). A covariance analysis did not demonstrate any difference between the treatment groups, in terms of changes in oxygen consumption. Oxygen consumption analyses was planned by Rowland, et al.(19), but due to technical equipment difficulties, gas exchange data was available in only five runners following the institution of iron therapy. As the group assignment of these five runners was not available from the published text, this parameter was not combined in the meta-analysis. No significant differences were observed in the iron or placebo treated subjects in maximal or submaximal oxygen consumption in this study. Treadmill endurance time After supplementing the subjects with iron for one month, Rowland, et al.(19) observed that the treadmill endurance time declined in every placebo treated subject (mean = –0.67 minutes, range = –0.07, –1.3). Amongst the iron treated subjects all except one improved their endurance times (mean = +0.57 minutes, range = + 0.03 to + 1.92). The girl in the iron treatment group whose endurance time did not improve had taken only 59% of her prescribed dose. The authors also observed a direct relationship between individual serum ferritin levels and change in treadmill endurance time during treatment (r = 0.74, p <0.05). Discussion The results from this data derived from three randomized controlled efficacy trials indicate that iron supplementation may have a positive effect on the physical performance of children. The post exercise heart rate was lower in the iron-supplemented group but not statistically significant. Significant benefits were observed with respect to the blood lactate levels and treadmill endurance time, estimated in one study each. However, two studies that estimated the oxygen consumption, showed no significant difference with iron supplementation. Some limitations merit consideration. First, is the limited nature of the data; we could identify only three trials comprising 106 subjects, which satisfied the inclusion criteria. The assessed quality of these three trials on various parameters was fair to good (Table I). Second, the studies do not provide information about other proximate factors affecting physical performance, like energy adequacy and freedom from morbidity, particularly infections. The contributions of these factors to the results are, at best, speculative. Third, the included trials have not provided information on other micronutrient deficiencies contributing to anemia; however, being randomized controlled trials, it can be assumed that these factors have been adequately accounted for. Fourth, one of the included trials had female adolescent athletes as the study subjects who received physical training for one month before the initiation of iron supplementation. The confounding effect of physical training, which is also likely to improve the physical performance, is speculative. Finally, in the absence of actually stated data on the variability of the change in outcome scores, imputations had to be done on the basis of pre-specified assumptions. The analyses suggest that these imputations were robust since the interpretation and quantification with various assumptions were invariably synchronous. A few interesting observations have emerged from this systematic review, which may have programmatic implications and can provide direction for future research. The pooled analyses did not show any significant effect of iron administration on post exercise heart rate in the study subjects. Previous studies in adults have shown that oxygen intake for a given workload and ventilation rate is similar irrespective of the hemoglobin status, but there is an increased cardiac output in anemic subjects due to an increased heart rate(21). After eliminating the one study(19) with iron deficient (serum ferritin < 20 ng/mL) but non-anemic subjects, the decline in heart rates following physical activity was seen to be statistically significant [(WMD = –13.L/ min (95% CI = –23.2, –3.1; P = 0.01), –14.2 /min (95% CI = –22.3, –6.1; P = 0.001) and –12.7 /min (95% CI = –23.5, –1.9; P = 0.021), at 5, 6 and 7 mph running speeds, respectively)]. Thus, the heart rate response to workload seems to be a sensitive monitor of hemoglobin and the oxidative capacity status of the body. Studies in older subjects have also documented an increase in hemoglobin and consequently, the physical capacity following iron supplementation(22-24). One study(15) documented a beneficial effect of iron supplementation on post exercise blood lactate levels. Several studies have documented a rise in the fasting blood glucose, increased production of lactate and adaptation of carbohydrate metabolism to increase the utilization of lactate as a metabolic substrate in the body(25, 26). With improvement in hemoglobin levels following iron supplementation, there is improvement in the oxygen carrying capacity. Therefore, the excessive conversion of pyruvate to lactate due to anerobiosis is decreased, bringing about a decrease in the blood lactate levels both before and after exercise(24). Thus findings of this review are in consonance with the results of similar studies conducted in adults(24). There was a significant improvement in treadmill endurance time with iron supplementation. Animal studies have suggested that endurance exercise capacity in iron deficient but non-anemic subjects is determined by oxidative capacity of the muscle and not the whole body oxygen consumption(27-29). Only subjects with decreased hemoglobin show decreased oxygen consumption(25,26). This phenomenon is probably related to the decreased mitochondrial enzyme activity and mitochondrial density in iron deficient subjects, and is probably responsible for the improved endurance times without any corresponding change in oxygen consumption in the iron deficient non anemic athletes evaluated by Rowland, et al.(19). Surprisingly, the African study, which evaluated oxygen utilization(14), showed no improvement with iron supplementation. The trial was conducted during a period when the availability of food was low and the transmission of malaria was high. There was a general deterioration in the running performance of the children in all the three treatment groups. Iron supplementation results in a lower hematological response in children residing in malarial areas (Sachdev HPS, Gera T). Effect of iron supplementation on hematological parameters in children: a systematic review of randomized controlled trials. Project Report of Research Project entitled Benefits of Iron Supplementation in Children: A Meta-analysis of Randomized Controlled Efficacy Trials, 2004, unpublished). Further, the contribution of other micronutrient deficiencies in these regions where malnutrition is widely prevalent and food security is scarce also needs evaluation. This review provides some direction for future research. In view of the paucity of controlled trials evaluating the role of iron supplementation on physical performance in children, there is an obvious need to generate relevant data. The simultaneous evaluation of iron levels and their correlation to physical performance needs greater attention. The effect of infectious illnesses, malnutrition and other micronutrients and vitamins on physical performance also needs evaluation while conducting such interventions. In conclusion, iron supplementation may have a positive effect on the physical performance of children, as evaluated through the post exercise heart rate, blood lactate levels and treadmill endurance time. In view of the limited data availability, this finding cannot be considered conclusive. Contributors: TG prepared the protocol, applied the search strategy, retrieved articles, and extracted the data. HPSS and PN conceived this review and finalized the protocol and search strategy. HPSS performed the statistical analysis. All the authors contributed to the drafting of the final version of the paper. HPSS and TG are the guarantors. Funding: The United States Agency for International Development through its cooperative agreement (No. HRN-A-00-98-00027-00) with the Human Nutrition Institute of the International Life Sciences Institute (ILSI) Research Foundation. The funding source had no influence on the study design, analysis and interpretation, and the decision to submit for publication. Competing interests: HPSS is an honorary member of the International Nutritional Anaemia Consultative Group (INACG) Steering Committee that is managed by ILSI. TG was supported by ILSI for travel to Hanoi, Vietnam, Marrakech, Morocco, and Lima, Peru for presenting research work in the annual INACG symposiums. PN was a consultant to ILSI.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()