|
|
Brief Reports Indian Pediatrics 2006;43:39-43 |
||||||||||||||||||||
|
Steroid Resistant Nephrotic Syndrome:Is Sustained Remission Attainable |
||||||||||||||||||||
|
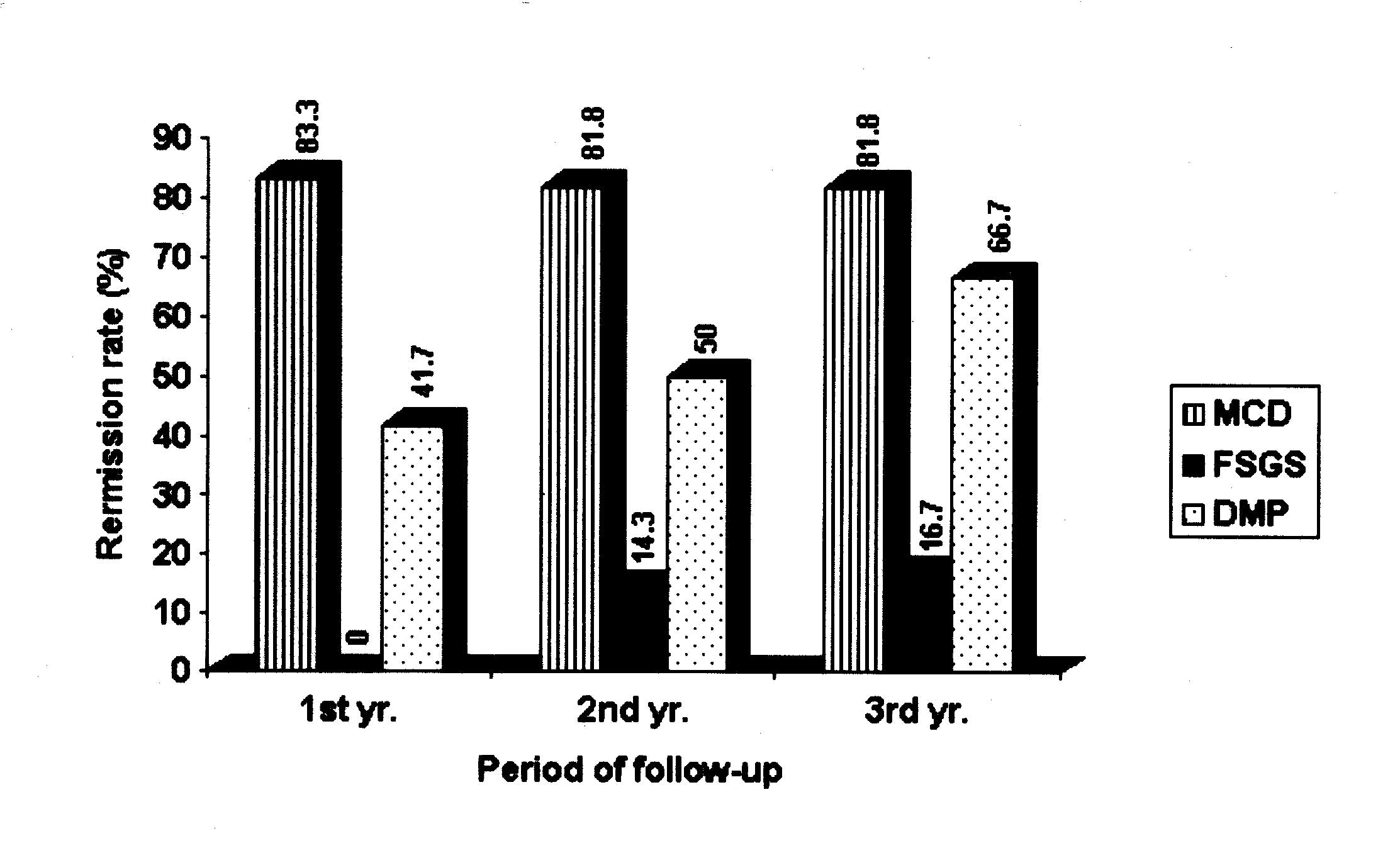
Idiopathic nephrotic syndrome (INS) is the most common glomerular disease in children. Most cases of INS in childhood have ‘minimal change’ histology and more than 90% will respond to steroids. Clinical non-responders include a heterogenous group comprising of histologically minimal change disease (MCD), focal segmental glomerulosclerosis (FSGS) and diffuse mesangial proloferation (DMP)(1). Ten per cent of children with INS develop steroid resistance (SRNS) and 50% of them will progress to end stage renal disease(2). Among non-responders, 25% or more have FSGS and half will progress to end stage renal failure, which constitutes about 10% of cases of end stage renal disease in children(1). It is this small group of nephrotic children who are treated with various modalities including steroids, other immunosuppressives, immunomodulators and antiproteinuric drugs. Cyclo-phosphamide and cylosporin are drugs frequently used in combination with prednisolone. This study utilized a treatment protocol that combined IV methyl prednisolone, IV cyclophosphamide and oral prednisolone for the treatment of SRNS. Subjects and Methods This prospective study was undertaken at the Department of Nephrology, Kanchi Kamakoti CHILDS Trust Hospital, Chennai from the year 1998-2002 to evaluate the efficacy of a treatment regime consisting of IV methylprednisolone, IV cyclophosphamide and oral prednisolone in children with SRNS and correlate the response in relation to histology. Nephrotic syndrome was defined as the presence of generalized edema, serum albumin <2.5 g/dL, serum cholesterol >220 mg/dL with proteinuria more than 3+ by dipstick, protein creatinine ratio >3.0 at 8.00 am urine specimen or urine protein >50 mg/kg/day. All these children received prednisolone at dose of 60 mg/m2/SA daily in single or 2 divided doses for 6 weeks followed by 40 mg/m2/SA on alternate days for 6 weeks. Steroid resistance was defined in this study as a failure to achieve resolution of clinical or laboratory features of nephrotic syndrome after 6 weeks of daily prednisolone therapy(3). All children with SRNS were included in the study. Children with documented SRNS but with clinical and laboratory pointers for secondary glomerulonephritis were excluded. These children had renal biopsy after obtaining parental consent. All the biopsies were interpreted by the same pathologist and were classified as MCD, FSGS and DMP. Forty-two children fulfilled the criteria and had renal biopsy and the following protocol of therapy. Of 42 children, 34 completed the course of treatment and are included in the study. Criteria for remission were urine protein one plus or less with urine protein creatinine ratio < 0.3. Therapy and monitoring These children were admitted and IV methyl prednisolone 30 mg/kg/day, diluted in 5% dextrose solution, given over 3 hours daily for 5 consecutive days followed by oral prednisolone 1 mg/kg on alternate days for one year. Intravenous cyclophosphamide was given on the 6th day at a dose of 750 mg/m2/SA, diluted in 5% dextrose, as an infusion over 3 hours. The dose of IV cyclophosphamide was repeated at monthly intervals for 5 more doses. Children were monitored for hypo-kalemia and diuretics were not given before institution of IV methyl prednisolone. Blood pressure and side effects of cyclophosphamide, including vomiting (Inj, ondansetrone was given prior to infusion), leukopenia, alopecia and hemorrhagic cystitis (administered drug in the morning and encouraging fluids if no edema) were noted. These children were followed up at frequent intervals with monitoring of their urine protein, blood pressure, blood counts, renal functions and infections. The time to onset of remission and maintenance of remission were noted in every child on follow-up. The end point of the study was at the end of one year of completion of oral steroids and subsequently at the end of second and third year without repetition of the protocol. Remission status was confirmed with the defined criteria. Serum creatinine level was considered as an indicator of renal function. Renal parameters like serum creatinine, serum albumin, serum cholesterol and calculated creatinine clearance were noted at the beginning and end of first, second and third year. During the second and third year, patients in remission received no drug treatment. Those who relapsed were treated with prednisolone at a dose of 60 mg/m2/day for 2 weeks followed by 4 weeks of 40 mg/m2 on alternate days. One child with FSGS was maintained on low dose prednisolone at a dose of 0.5 mg/kg on alternate days for 8 months during second year as child was showing non nephrotic proteinuria at the end of one year. Angiotensin converting enzyme inhibitors and angiotensin receptor blockers for their antiproteinuric effects were used in patients during second and third year follow up. No other drugs like azathioprine, cyclosporin A or mycophenolate were used during three years. Results Of 34 children, 13 (38.2%) were boys and 21 (61.8%) were girls. Seventeen (50%) patients were in the age group of 2-5 years and 8 (23.5%) were above 5 years of age. Hypertension was present in 23.5% of the children and 20.6% had hematuria. Renal failure was noted in 11.8% of the children, with serum creatinine ranging from 1.3 mg/dL to 1.6 mg/dL. Twelve patients (35.5%) each had either MCD or DMP, 10 (29.4%) had FSGS. After IV methyl prednisolone and first dose of IV cyclophosphamide, no child went into remission by one month. Among those who subsequently went into remission following therapy, 86.7% were in remission by 4th dose of IV cyclophosphamide and one child each went into remission by fifth and sixth doses of IV cyclophosphamide respectively. At the end of one year, 83.3% with MCD, 41.7% with DMP and none with FSGS were in remission. By the end of second year 81.8% of MCD and 50.0% of DMP were in remission. Of seven patients with FSGS followed up to 2 years, one showed remission with low dose alternate day oral prednisolone therapy during the second year. Remission status at the end of three years from the time of starting the therapy is given in Table I. In FSGS out of 6 children followed up to 3 years, 5 (83.3%) continued to be proteinuric. Patients with MCD did not show a change in the remission status. In DMP one more child showed remission with oral steroids increasing the percentage of remission to 66.7%. Remission rates at three years were 16.7% in FSGS, 81.8% in MCD and 66.7% in DMP (Fig.1). It should be noted that the number of children who were lost to follow-up skews findings particularly in FSGS.
TABLE I–Remission Status at the End of Third Year Based on Histology.
Side effects like leukopenia, hypertension, dysuria and hemorraghic cystitis were not seen in any patients. Following IV cyclophosphamide, no child had deterioration of renal function. Infectious episodes during the study and follow-up, were 22 of which 5 were very serious. Three had septicemia, two each had pneumonia and cellulitis and one child had urinary tract infection. Other minor infections included upper respiratory tract infection and minor skin infection. Except two children, all of them had normal hair growth and even the two children who had episodes of hair falling improved with improvement of serum albumin levels. Those children with renal failure at the beginning of the study showed a reduction in the renal failure status at the end of one year with only one child showing persisten t renal failure with serum creatinine ranging from 1.2 to 1.4 mg/dL on follow-up for 3 years. No significant differences were noted with serum creatinine and calculated creatinine clearance in other children. There was satisfactory decrease in mean serum levels of cholesterol from 362 ± 122 mg/dL to 264 ± 96 mg/dL. Similar response was noted with serum albumin following treatment with mean level increasing from 1.8 ± 0.6 g/dL to 2.8 ± 0. 7 g/dL. Discussion The need for many therapeutic trials for SRNS indicates that final word has not been said(3-12). Hence, we conducted this study with the regime mentioned. Fifty percent were in the age group of 2-5 years and the peak age incidence of both MCNS and FSGS is in pre-school children. According to ISKDC, 80% are less than 6-years old at presentation with median age at diagnosis being 2.5 years for MCD and 6.8 years for FSGS(13). However in our study majority of the children were less than 5 years (76.5%). No particular age pre-disposition in relation to histology could be made. There was preponderance of female children with male to female ratio of 1 : 1.6. This gender preponderance of female has not been discussed in previous studies on SRNS. Hypertension (23.5%), hematuria (20.6%) and renal failure (11.8%) were more common than that described for primary nephrotic syndrome(14). On histology, 35.3% each had MCD or DMP followed by FSGS in 29.4% of children. The remission rate at the end of three years was 16.7% in FSGS, 81.8% in MCD and 66.7% in DMP, with the number of children who were lost for follow-up skews findings particularly in FSGS. This is in contrast to the claims made in various studies particularly in FSGS where complete remission was documented in 70% by Rennert, et al., 40% by Adhikari, et al. and 65% by Gulati, et al. on varying periods of follow-up(7,15,16). In our series it was 16.7% in FSGS, which may be due to various reasons; one child had died before first year of life due to septicemia and 3 more children were lost for follow-up by third year. Contrastingly, in MCD, 83.3% of the children were in remission at the end of one year and this better status continued with 81.8% at the end of second and third year and is comparable to 100% complete remission reported earlier. This is contrary to the study done by Bajpai, et al. wherein remission rates were lower in the MCD and higher in the FSGS group following IV cyclophosphamide and oral steroids(18). In this study, 16 out of 26 (61.5%) had sustained remission at the end of third year of followup compared to 7 out of 24 (29.2%) after a followup of 1.8 ± 0.4 years by Bajpai, et al.(18). Contributors: BRN, MVK, NP and DVJ were involved in care of the patients. MVK and NP prepared the manuscript and BRN reviewed the manuscript. BRN will act as the guarantor for the paper. Funding: Research grant given by Medical Research Foundation of Kanchi Kamakoti CHILDS Trust Hospital, Chennai 600 034. Competing interests: None stated.
| ||||||||||||||||||||
|
References | ||||||||||||||||||||
|
|
![]()