|
|
Original Article Indian Pediatrics 2006; 43:20-25 |
||||||
|
Does End-tidal Carbon Dioxide Measurement Correlate with Arterial Carbon Dioxide in Extremely Low Birth Weight Infants in the First Week of Life? |
||||||
|
Soraisham Amuchou Singh and Nalini Singhal From the Department of Pediatrics, University of Calgary, Alberta, Canada. Correspondence to: Dr. S. Amuchou Singh, Department of Pediatrics, Foothills Hospital, C-211, 1403, 29th Street, NW, Calgary, Alberta-T2N2T9, Canada. E-mail: amuchou@yahoo.com Manuscript received: April 7, 2005, Initial review
completed: May 25, 2005,
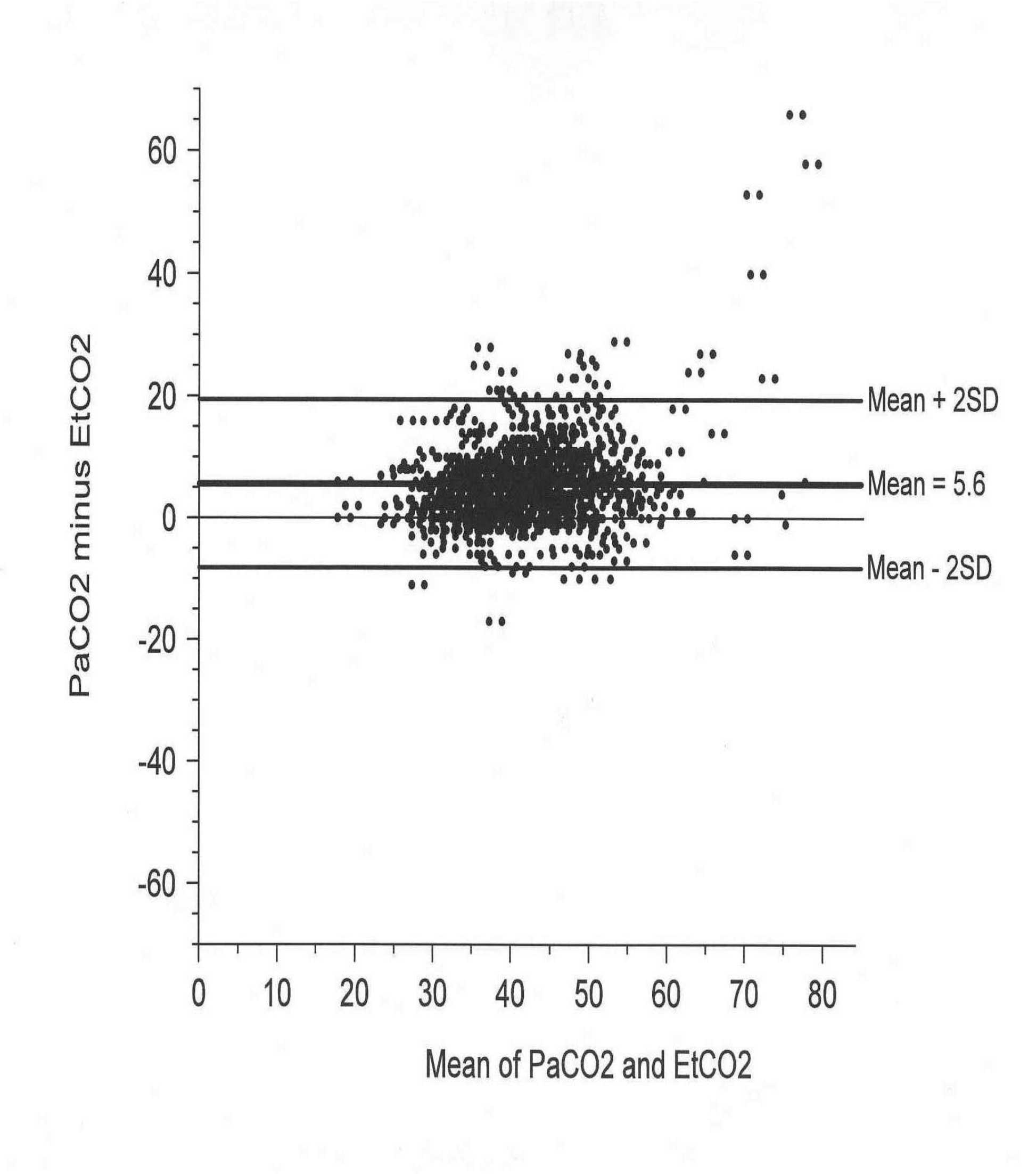
Objective: To study the correlation and agreement between end-tidal carbon dioxide (EtCO2) and arterial carbon dioxide (PaCO2) in ventilated extremely low birth weight (ELBW) infants in the first week of life. Methods: Retrospective chart review of all ELBW (<1000 g) infants admitted to a level III NICU from January 2003 to December 2003. Data collected included demographic details and simultaneous EtCO2 (mainstream capnography) and arterial blood gas values (pH, PaCO2, PaO2). Outcome: The correlation coefficient, degree of bias with 95% confidence interval between the EtCO2 and PaCO2. Results: There were 754 end-tidal and arterial CO2 pairs from 31 ELBW infants (21 male and 10 female). The overall EtCO2 values were significantly lower than PaCO2 value (EtCO2=37.3 ± 7.8 mmHg Vs PaCO2=43.5 ± 9.6 mmHg, P<0.0001). In only 89/754(11.8%) pairs, the EtCO2 was higher than the PaCO2. The overall bias was 5.6 ± 6.9 mmHg (95% C.I. 5.11-6.09). The intraclass correlation coefficient was 0.81. Using EtCO2 ranges of 30 to 50 mmHg, the capnographic method was able to identify 84% of instances where PaCO2 was between 35 (<35 = hypocarbia) and 55 mmHg (>55= hypercapnia). Conclusions: There is good correlation and agreement between end-tidal CO2 and arterial CO2 in ELBW infants in the EtCO2 range 30-50 mmHg. End-tidal CO2 monitoring can be helpful in trending or for screening abnormal PaCO2 values in ELBW infants in first week of life. Key words: Capnography, End-tidal carbon dioxide, ELBW, PaCO2. Arterial blood gas analysis is essential for monitoring the adequacy of ventilation and oxygenation in ventilated babies. It is often difficult to obtain arterial blood gases frequently especially where resources are limited. Arterial blood sampling leads to blood loss, pain, stress and arteriospasm in neonates and hence need for non invasive monitoring. Pulse oximetry provides the non-invasive method of assessing the oxygenation in neonatal intensive care unit (NICU) patients(1) It is necessary to have a reliable, non-invasive method for detecting hypocarbia and hypercarbia. Both hypocarbia and hypercarbia are detrimental to the ELBW infants and have been implicated as a causative factor in periventricular leukomalacia (PVL), intra-ventricular bleed (IVH) and chronic lung disease (CLD)(2-7). Maintaining the PaCO2 within the desired range by frequent arterial sampling can increase the need for multiple transfusions in these infants(8). Transcutaneous CO2 monitoring is a non-invasive technique for measuring the carbon dioxide(9). However, transcutaneous CO2 monitoring is not tolerated in VLBW infants because of their fragile skin and is affected by acidosis and hypoxia(10). End-tidal carbon dioxide (EtCO2) measurement by capnography is a continuous and non-invasive indirect measurement of blood carbon dioxide tensions. Capnography is done by either side-stream or mainstream gas sampling. The technique, which measures the concentration of CO2 in exhaled gas, has been used extensively in adults and children(11,12) The reliability of mainstream capnography has also been reported in term and preterm neonates(13-15). The EtCO2 monitoring has some clear advantages over the transcutaneous CO2 monitoring, such as a much faster response time to changes in blood CO2 levels, internal calibrating ability and no thermal injury to the fragile skin of the newborn(16). This noninvasive method can reduce the blood loss and pain associated with arterial blood gas sampling. This study was done to find out the correlation and agreement between EtCO2 and arterial CO2 in ventilated ELBW infants in first week of life. Subjects and Methods This study is based on a retrospective chart review of all ELBW babies admitted in a level III NICU in Southern Alberta over one year period (January 2003 to December 2003). The data are derived from a quality improvement study to audit the usefulness of EtCO2 monitoring in the ELBW babies. ELBW babies (<8 days) receiving mechanical ventilation who had indwelling arterial catheter and end- tidal CO2 monitor by mainstream capnography were included in the study. Babies with structural cardiopulmonary malformation and those ventilated on high frequency ventilation were excluded from the study. Demographic details, gestational age, birth weight, details of surfactant therapy, simultaneous EtCO2 and arterial blood gas values (pH, PaCO2, PaO2) along with ventilatory settings were retrieved from the case record. Exhaled CO2 was continuously monitored by using a commercially available mainstream capnography (Capnogard ETCO2 monitor, Model 1265, Novametrix Medical Systems Inc, Wallingford, Connecticut, USA). This device measures changes in the CO2 concentration of the infants exhaled tidal volume, which is passing through an airway adapter containing capnostat sensor. Infrared light is generated in one leg of the U shaped sensor and then beamed through the windows of the airway adapter to a detector in the other leg of the sensor. The adapter (< 0.5 mL dead space) is placed just proximal to the endotracheal tube. The capnograph was calibrated everyday according to the manu-facturer’s recommendations. The arterial blood gas analysis was performed on blood obtained from the indwelling arterial catheters via umbilical or radial arteries, using an automatic blood gas analyzer (Radiometer ABL 725 Operation) that was calibrated daily. To determine whether EtCO2 were representative of PaCO2, the relationship between the end-tidal and arterial CO2 was analyzed by simple linear regression. The precision of the EtCO2 and the agreement between EtCO2 and PaCO2 (gold standard) were assessed by bias, standard deviation and calculating the 95% confidence interval (CI) for the bias (bias = PaCO2-EtCO2)(17). Data were correlated using intraclass correlation coefficient. Differences between EtCO2 and PaCO2 were compared by using paired "t" test. Values were express as mean ± SD of the mean (and range when appropriate). A statistically significant difference was defined as p <0.05. Results Thirty-one ELBW infants (21 boys and 10 girls) were included in the study. The mean birth weight was 740 ± 130 g (range 500- 970 g) and the mean gestational age was 25 ± 1 weeks (range 23-27 wk). All infants had hyaline membrane disease and treated with surfactant. All infants were ventilated using pressure-limited, time-cycled ventilators in a variety of modes, including intermittent mandatory ventilation and synchronized intermittent mandatory ventilation (Infant star and Drager Babylog 8000 ventilators). A total of 754 EtCO2-PaCO2 pairs were available for analysis from 31 infants. The overall EtCO2 was significantly lower than the corresponding PaCO2 values (EtCO2 = 37.3 ± 7.8 mmHg vs PaCO2= 43.5 ± 9.6 mmHg respectively, P <0.001). In 89/754 (11.8%) pairs, the EtCO2 was higher than the PaCO2. Figure 1 shows the scattergram of the end-tidal CO2 and PaCO2. Pearson correlation coefficient was 0.71.The overall EtCO2 bias was 5.6 ± 6.8 mmHg with a 95% confidence interval for mean of 5.11-6.09. The bias in the relationship between the EtCO2 and PaCO2 is illustrated in Fig. 2 where the difference is plotted against the average of the two values (Bland-Altman Plot). There was a good agreement between EtCO2 and PaCO2 with the intraclass correlation coefficient of 0.81 (P <0.0001).
Using end-tidal CO2 ranges of 30 to 50 mmHg, the capnographic method was able to identify 84% of instances where PaCO2 was between 35 (<35 = hypocarbia) and 55 mmHg (>55 = hypercapnia). When the end-tidal CO2 is beyond the limit i.e., EtCO2 <30 mmHg (n = 87) or >50 mmHg (n = 49), capnographic method was able to identify 78/136 (57.3%) of instances where PaCO2 was <35 mmHg (51/87) and PaCO2 >55 mmHg (27/49). Discussion This study showed that there is a good correlation and agreement between EtCO2 and PaCO2 in surfactant treated, ventilated ELBW babies during the first week of life. Although arterial blood gas analysis remains the most accurate method of ascertaining blood CO2 tensions, alternative non-invasive methods are crucial and desirable because these infants have limited blood volumes and frequent blood gas sampling contributes to the high transfusion rates seen in ELBW infants. The need to quickly assess and respond to changes in CO2 pressures has become more critical with the increased recognition that both low and high PaCO2 for even brief periods of time are associated with long term morbidity in these patients. Rozycki, et al.(13) and Wu, et al.(14) reported a good correlation between the EtCO2 and PaCO2 in neonates including preterm babies. These authors suggested that EtCO2 monitoring by mainstream capnography was accurate method for trending and screening infants with abnormal PaCO2. In the pre surfactant era, EtCO2 monitoring was reported to be unreliable for estimating PaCO2 in preterm babies with respiratory distress(15). Nangia, et al.(15) also reported similar findings in preterm babies with hyaline membrane disease. The poor correlation may be due to small sample size, different devices for exhaled CO2 monitor and use of side stream capnography(15,16). Other published studies have shown that factors such as poor cardiac output, hypothermia, size of tidal volume and lung disease (especially if an increased in dead space is present) adversely affect the EtCO2-PaCO2 relation-ship(16,18,19) The EtCO2 is usually lower compared to corresponding PaCO2. The consistent bias of the EtCO2 value in this study is within the range reported in previous studies of main stream capnometry in neonates(13,14). The lower value for the end-tidal measurement may be attributable to gas mixing proximal to the endotracheal tube. End-tidal carbon dioxide measurement from gas sampled distally to the endotracheal tube-ventilator connection more closely matches the arterial value(20,21). The severity of lung disease, the ventilation index and the oxygenation index had negligible influences on the degree of bias(13). The normal range of carbondioxide to be maintained during assisted ventilation is 35 mmHg to 55 mmHg. Hypocapnia and hypercapnia are harmful to the brains of preterm and term infants. There is a strong association between PaCO2 values less than 25 to 30 mmHg and an increase incidence of cystic periventricular leukomalacia, periven-tricular echo densities or chronic lung disease in preterm infants(2-7). The upper limit of benign PaCO2 levels is less clear. In a randomized trial of permissive hypercapnia, mild hypercapnia (PaCO2 45-55 mmHg) did not increase the incidence of IVH in VLBW infants(22). However, severe hypercapnia (PaCO2 >60 mmHg) was associated with intraventricular hemorrhage in a large retrospective study(6). The goal of mechanical ventilation should be avoiding hypocapnia or hypercapnia, rather than achieving a specific level or range of PaCO2. Hence, the continuous noninvasive monitoring of CO2 by capnometry is helpful in these vulnerable preterm infants. Based on this approach, we have demonstrated that the mainstream end-tidal CO2 monitor will indicate that the PaCO2 is within prescribed parameters (PaCO2 between 35 and 55 mm Hg) 84% of the time. Since this study consisted of retrospective data collection, data regarding the waveform, its characteristics or changes in the waveform were not recorded in this study. However, it is not known in the literature that the addition of wave form analysis to the EtCO2 value would improve the ability of the end-tidal CO2 monitor to act as a warning device that the PaCO2 is approaching undesirable levels. Other limitations is that when the end-tidal monitor was outside the prescribed limits (EtCO2 <30 or >50 mmHg), the PaCO2 was truly in the hypocapnia (PaCO2 <35 mm Hg, 51/87) or hypercapnia (PaCO2 >55 mm Hg, 27/49) range in 78/136 instances (57.3%). On the other hand, out of 640 instances where PaCO2 was >35 mmHg, there were only 31 instances where EtCO2 value was <30 mmHg. [i.e. specificity 609/640 (90%)]. In summary, we found good correlation and agreement between EtCO2 and PaCO2 in ventilated ELBW infants during the first week of life. We suggest using the EtCO2 measurement to adjust ventilator settings when the monitor is within the range of 30 to 50 mmHg but recommend periodic check of blood gases to make sure it is within normal range of PaCO2, and to obtain arterial blood gases when the end-tidal monitor shows readings beyond these limits. This protocol may reduce the amount of barotrauma by allowing for more prompt adjustment of the ventilatory settings in response to changes in PaCO2. It may also reduce the exposure time to hypocapnia and hypercapnia and therefore decrease the brain injury; and finally it may reduce the number and total volume of blood samples required for gas measurement. Contributors: SAS plan the study, collected the data and drafted the manuscript. NS supervised the drafting of the manuscript. SAS would act as the guarantor of the paper . Funding: None. Competing interests: None.
| ||||||
|
References | ||||||
|
|
![]()