|
|
Letters to the Editor Indian Pediatrics 2005; 42:84-86 |
||
|
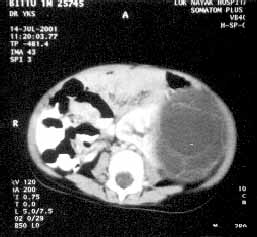
Cystic Nephroma |
||
|
Patient was managed by nephrectomy. Histopathological examination revealed multilocular lesion with definite epithelial lining of loculi. There was no solid tissue identified within the cystic tumor. Neither mature nephrons nor malignant blastemal cells were present within the septae of the cystic lesion. Loculi were neither communi-cating with each other, nor with renal pelvis. Rest of the kidney was normal except for slight pressure atrophy. The histopathological diagnosis was Cystic Nephroma (CN). No adjunct therapy was administered. On follow-up, he is free of any recurrence one year and six months after the surgery. CN is uncommon, non-heritable, unilateral, benign tunor that represents 2-3% of primary renal tunors in the pediatric age group(1). CN has a bimodal incidence with 50% of tumors presenting in children younger than 4 years of age(2). In this age group, boys predominate in a ratio of 2:1. The second peak incidence occurs in adults and unlike the pediatric cases, is usually seen in women. CNs are commonly found incidentally on radiographic studies, but may present as an abdominal mass found on routine physical examination. The differential diagnosis of cystic nephroma include multicystic dys-plastic kidney, a very necrotic or hemorrhagic Wilms’ tumor, clear cell sarcoma, or a cystic variant of mesoblastic nephroma. On ultrasound, CT and MRI, CN appears as an encapsulated multilocular cystic mass. In contrast enhanced CT scan, the septa may enhance but cysts remain low in intensity. Similarly, in MRI, gadolinium administration enhances septa but not the cysts(3). Grossly, CN is characterized by a segmental, purely cystic-well circumscribed mass that may partially replace the renal parenchyma. It is characterized by multiple septations entirely of differentiated tissue without blastemal elements. Cystic nephroma and cystic partially differentiating nephro-blastoma (CPDN)/solid nephroblastoma (Wilms’ tumor) represent benign and malignant ends of a spectrum respectively, however exact relationship between these entities is not known and is rather controversial. Differentiation between these entities has a prognostic and diagnostic significance. CN is the most differentiated form in the spectrum. To lable a lesion to be a cystic nephroma, presence of blastemal cells and poorly differentiated cells should be ruled out. Cystic nephroma is a benign lesion, which is cured by nephrectomy. Recurrence has occurred following incomplete excision by partial nephrectomy(4). If partial nephrectomy is considered, frozen section is indicated to exclude cystic, partially differentiated nephroblastoma(5). Y.K. Sarin, | ||
|
References | ||
|
|
![]()