|
|
Case Reports Indian Pediatrics 2002; 39: 92-95 |
||||||||||||||||||||||||||
|
Primary Fetal Hydrothorax |
||||||||||||||||||||||||||
|
Ramesh Agrawal Rajiv Aggarwal Alka Kriplani* Neerja Bhatla*
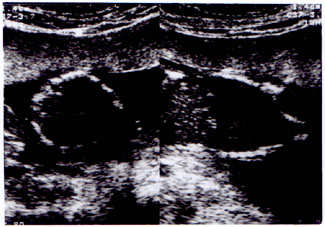
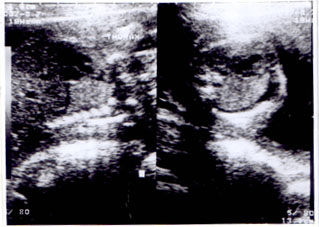
Primary Fetal Hydrothorax (PFHT) or fetal chylothorax, is an intrathoracic collec-tion of fluid in the fetus, which may be present on either side or even bilaterally. This is a rare anomaly occurring in 1 in 10,000 - 15,000 pregnancies. The clinical course of PFHT is highly variable with outcomes varying from spontaneous regression to fetal or neonatal death(1,2). Although, this condition has been reported in Western literature, awareness regarding PFHT and its management is missing in Indian reviews. We report two cases of PFHT and review its management. Case Report Case 1 A 24-year-old primigravida was referred to our hospital with an antenatal diagnosis of left sided pleural effusion in the fetus at 17 weeks of gestation. This pregnancy was a spontaneous conception and was otherwise uneventful. Blood group of the woman was O positive with B positive husband. Her TORCH screen and VDRL tests were negative. She had been advised termination of pregnancy outside. At our hospital, a repeat ultrasound con-firmed the above finding (Fig. 1). Underlying lung parenchyma was normal. There were no changes suggestive of hydrops or any other malformation. Fetal growth and liquor were adequate. Fetal cardiac echocardiography revealed normal structure and rhythm. The case was discussed in the perinatal meeting and a decision to continue the pregnancy was taken. A repeat ultrasound was planned after 3 week. The repeat ultrasound at 20 week showed complete resolution of effusion. No recurrence was noted thereafter till delivery. At 37 week, she delivered a female baby weighing 2.6 kg. The baby did not require any resuscitation. Postnatal course was un-eventful. There were no obvious mal-formations. Chest X-ray did not reveal any effusion and lung parenchyma was normal. Case II The second case was an uneventful pregnancy in a 30-year-old, second gravida woman. An antenatal ultrasound at 22 weeks detected a significant pleural effusion on the left side in fetus, causing minimal displace-ment of the mediastinum to the contralateral side. The underlying lung parenchyma was normal (Fig. 2). There was no poly-hydramnios or changes suggestive of hydrops in the fetus. There were no other malforma-tions and fetal growth was adequate. Her blood group was B positive. Her VDRL test and TORCH screen were negative. It was decided to continue the pregnancy and to keep her under follow up. At 24 weeks, there was complete resolution and no recurrence of effusion occurred thereafter till delivery. She delivered a healthy female baby (birth weight 3.49 kg) with normal Apgar scores. There was no malformation in the baby and postnatal course was uneventful.
Fig. 1. Antenatal ultrasound showing massive effusion on left side with mediastinal shift (Case I).
Fig. 2. Antenatal ultrasound showing significant pleural effusion on the left side. Discussion Fetal hydrothorax or pleural effusion is a clinical entity, which may be idiopathic (primary) or secondary to a variety of disorders such as cardiac, pulmonary and gastro-intestinal malformation, infection, hematological and chromosomal abnormali-ties or as part of immune hydrops(3). It is a rare disorder but with increased awareness and widespread usage of antenatal ultrasound, fetal pleural effusion is likely to be diagnosed more frequently. However, the natural history of this disease entity is not well understood and the prognosis remains variable. The perinatal mortality associated with pleural effusion is at least 50%(2).
The first case of fetal pleural effusion was described by Carroll(4). Aubard et al.(2) conducted a meta-analysis on cases with primary PFHT reported in English and French literature between 1977 and 1996. The investigators included 204 cases reported in 64 different publications. The mean time of detection was 27.3 (±5.6) weeks of gestation. Most of the cases (75%) were detected during the third trimester although a few cases were detected as early as 13 weeks of gestation. The clinical course in these patients was quite variable with spontaneous resolution occur-ring in 22% cases, favorable outcome after treatment in 43% and poor outcome (fetal/neonatal death) in 35% cases. Cases with unilateral pleural effusion, earlier detection (early second trimester), absence of poly-hydramnios and hydrops were more likely to undergo spontaneous resolution. Bad prog-nostic factors included an increase in fluid volume, involvement on both sides, poly-hydramnios and hydrops and these were associated with poor outcome. On multi-variate analysis, hydrops was the only factor, independent of bilateral effusion and gestational age at the time of delivery, responsible for predicting poor outcome. The therapeutic approach adopted in the management of PFHT is dependent upon the clinical presentation. Presence of fetal distress is a medical emergency and should be managed with urgent fetal thoracocentesis. This procedure is safe and effective in an emergency. The principal drawback in this procedure is the rapid re-accumulation of fluid. Once the fetus is stabilized, further evaluation should be done to confirm the diagnosis of PFHT. Secondary causes of PFHT and any associated fetal anomaly should be excluded (Tables I & II). If an effusion is unilateral and well tolerated, a conservative approach should be taken and a repeat ultrasound should be done after 2-3 weeks. If regression or stabilization has occurred, then the patient should be kept under follow-up with regular ultrasounds. In the event of worsening or appearance of any bad prognostic factors, subsequent management would depend upon the period of gestation. Pleuro-Amniotic Shunting (PAS) involves placement of a catheter draining pleural fluid into amniotic cavity(2,5,6). Shunting is recommended if the pregnancy is less than 32 weeks. Failure despite repeated attempts is always associated with poor prognosis and termination of pregnancy may be advised in such cases. If pregnancy is more than 32 weeks, fetal thoracocentesis can be under-taken since it is less invasive and has better efficacy when done between 32 and 37 weeks as compared to an earlier gestation. It is recommended that thoracocentesis should be performed in all cases with residual fluid near term in order to facilitate proper lung expansion after birth. The objective of presenting these two cases was to increase awareness about this common disease entity among pediatricians and obstetricians. With increasing use of antenatal ultrasound screening, an increasing number of fetal pleural effusions are likely to be diagnosed. Awareness regarding the good and bad prognostic factors would be helpful in counseling and early referral of the mother. Being aware of a recommended schema for the management of this condition would help in alleviating unnecessary anxiety among the parents and physicians. At the same time there is a need to develop expertise in various tertiary perinatal centers to conduct proce-dures such as thoracocentesis and pleuro-amniotic shunting. Contributors: AK and NB did the obstetric work up while RMA and RJA were responsible for the neonatal work up and follow up. RMA and RJA drafted the manuscript. AK and NB critically reviewed the manuscript. RJA would act as the guarantor for the paper. Funding: None. Competing interests: None stated.
References
|
|
|
![]()