|
|
Case Reports Indian Pediatrics 2002; 39: 88-91 |
||||
|
Unusual Presentation of Disseminated Tuberculosis |
||||
|
Munni Ray Sudha Kataria* Pratibha Singhi
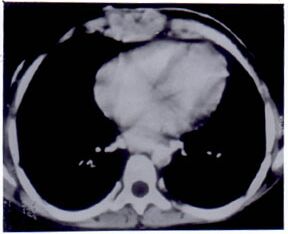
Extra pulmonary tuberculosis and skeletal disease in particular, may be of insidious onset and often pose a diagnostic challenge. Rarer still is the association with skin, ocular and lymph nodal tuberculosis. We hereby report an unusual case of disseminated tuberculosis with uncommon sites of involvement. Case Report A 10-year-old girl presented with history of painless nodular skin eruptions over the anterior chest wall, neck and left axilla for past one year. These lesions initially pea sized, enlarged, suppurated and ulcerated dis-charging pus. Some of these lesions healed spontaneously by scarring. Progressive deformity of the chest wall was noted for the last six months. A similar discharging lesion appeared over the left eyelid for two months prior to presentation to the hospital and she was unable to close her left eye. There was history of progressive weight loss and low-grade intermittent fever for six months. She had received several courses of oral antibiotics and local ointments from private practitioners prior to reporting to our hospital. She was BCG vaccinated and there was no history of contact with tuberculosis in the family. The patient was alert with no acute distress. Her height was 120 cm and weight as 20 kg (both <3rd centile). Vital signs were normal. Examination of skin over the anterior chest wall, neck and left axilla revealed widespread ulcerations and discharging sinuses with dusky red discoloration of bases (Fig. 1). Skin at some places was attached to the underlying structures, indurated and fibrosed. Cervical and axillary lymphadenopathy was present. Ectropion of the left eye was detected along with a discharging wound over the left eyelid. Schirmer’s test done to rule out involvement of the lacrimal gland was negative. On chest examination pectus carinatum was noted and breath sounds were normally heard over both lung fields. There was no hepatosplenomegaly. Cardiovascular and neurological examinations were within normal limits. Laboratory data included a hemoglobin of 6.7 g/dl, white blood cell count of 15,000/mm3 with normal differential count and platelets of 6.48 lacs/mm3. The erythrocyte sedimentation rate was elevated and HIV test was negative. Tuberculin skin test was positive with 20 × 25 mm induration with vesiculation. The posteroanterior view of the chest X-ray was normal but the lateral view revealed destruction and replacement of the lower end of the sternum by a soft tissue mass. Computed tomography of the chest revealed destruction of the body of the sternum with substernal abscess (Fig. 2). Patchy nodular ill-defined densities in the lung parenchyma were noted bilaterally. Paratracheal nodes were also enlarged. Skull X-ray revealed a sclerotic superior margin of the left orbit. Computed tomography of the left orbit indicated involvement of the roof of the left orbit. Pus from the skin lesions was sterile and no acid-fast bacilli (AFB) could be demonstrated both on staining as well as culture. Skin biopsy revealed chronic inflammation in the perivascular adenexal regions of the dermis. No evidence of granulomatous reaction in the dermis was noted. Stain for AFB was negative. Polymerase chain reaction for detecting Mycobacterium tuberculosis DNA on formalin fixed, paraffin embedded tissue was positive. Fine needle aspiration cytology from left axillary node revealed multiple epithelioid granulomas but stain for AFB was negative. The family screening was negative.
Fig. 1. Scrofuloderma over the anterior chest wall, neck and left axilla.
The patient was diagnosed as having tuberculosis and treated with isoniazid, rifampicin, pyrazinamide and ethambutol for two months. The skin and eyelid lesions healed and the child was continued on isoniazid and rifampicin for 10 more months. Thereafter the child underwent oculoplasty for management of ectropion. Discussion This case presented with a combination of various unusual types of tuberculosis, viz., skeletal–especially sternal and cranial osteomyelitis, ocular particularly palpebral involvement along with skin. Only 1.5% of children with tuberculosis have skeletal involvement, mainly the spine and the major weight bearing joints. Multifocal skeletal disease is uncommonly reported in children and unlike in adults they involve the peripheral skeleton more commonly than the axial skeleton(1,2). In the index case, however, the axial skeleton was affected. Tuberculous osteitis occurs secondary to lymphohemato-genous dissemination at the time of initial pulmonary infection with local reactivation at a later date. Isolated involvement of bone without spread to a joint fails to draw attention as well as subtle symptomatology delays the diagnosis as depicted by our case. Martini et al reported that the average delay in diagnosis was 28 months(3). Sternal tuberculosis represents less than 1% of tubercular osteomyelitis. It can arise due to either direct extension from hilar lymph nodes or hematogenous or lymphatic dissemination. In our case the mode of spread could be hematogenous as there was no radiographic evidence of contiguous spread from the nodes or lung parenchyma. Computed tomography of the chest is more useful in determining the extent of osseous destruction and involvement of soft tissue masses in cases of chest wall abscess(4). It is also helpful in demonstrating lung parenchymal lesions when chest radiography fails to do so(5), as was seen in our case. Only few case reports of sternal tuber-culosis are present in pediatric literature(6,7). Calvarial tuberculosis is a rare presentation and occurs in less than 1% cases of skeletal tuberculosis. The frontal and parietal bones are commonly involved because of presence of large amounts of cancellous bone. Occipital and sphenoid bones are rarely involved. When the outer table of the cranium is involved, tuberculosis might present as a subgaleal swelling or a discharging sinus. Involvement of the inner table is usually associated with formation of underlying extradural granulation tissue. In our case outer table involvement was present. Three types of lesions have been described on plain X-ray: perforating, diffuse and sclerotic form of tuberculosis of the cranium(8). The third type, which was present in our case, is the least common type of lesion. Ocular involvement in patients with tuberculosis is uncommon. In India systemic tuberculosis is rampant but ocular tuberculosis is a rarity(9). Eye involvement is usually found in healthy individuals with healed focus unlike in our case. It is rare in patients with frank pulmonary tuberculosis. It may involve any part of the eye and have different clinical forms. Uveal tract (the choroid and occasion-ally the iris) is the most frequently involved. Retinal involvement may present as exuda- tive lesions and/or as central or peripheral vasculitis(10). Affection of adenexal structures like lid and orbit as was present in our case is extremely rare. Cutaneous tuberculosis represents 1.5% of all cases of extra pulmonary tuberculosis worldwide(11). An upward trend of cases with skin tuberculosis has been noted in recent years. Misdiagnosis, neglect or late diagnosis in children may result in extensive disease due to lack of awareness of practitioners or scant attention by elders as was seen in our case(12). Several classifications of this disease are available. A recent modification cited by Kumar et al. suggested that this disease could primarily be classified into three categories:(i) localized disease, (ii) disseminated disease; and (iii) tuberculids(11). Our case would qualify for a disseminated disease as skin involvement was present with another system involvement. Scrofuloderma is the commonest form seen in children, especially in girls and results due to breakdown of skin overlying a tuberculous focus either in the lymph node or in the bone. Often diagnostic difficulty is faced in labeling this condition. Clues to diagnosis rest upon the morphological identification, positive Mantoux test and any other focus of infection in the body. Skin DNA polymerase chain reaction has improved the diagnostic accuracy but exact sensitivity and specificity of this test is not yet fully known(13). BCG vaccine offers protection against dis-semination of tuberculosis especially against meningeal involvement but not pulmonary tuberculosis. Although our patient received BCG vaccine she developed both pulmonary as well as extra pulmonary disease. There is still no consensus on the optimal therapy of chest wall tuberculosis. While some authors conclude that it is a surgical entity, others opine that combination antituberculosis chemotherapy should be the mainstay of treatment. Only a small proportion of abscesses need repeated aspirations and surgical incision and excision may not be necessary(14). Calvarial tuberculosis is also managed with chemotherapy and surgery is indicated only in cases involving large extradural collections causing neurological deficits, associated fulminating infections, associated sinus formation and large pockets of caseating materials(8). Standard chemotherapy schedule is recommended for management of all forms of cutaneous tuberculosis(11). Awareness of the unusual presentations of tuberculosis is essential for early diagnosis and proper therapy. Contributors: MR carried out the clinical work up and also drafted the manuscript. SK was responsible for the radiological aspects and co-drafted the manu-script. PS was the consultant in charge of the patient and supervised drafting of the paper. She will act as the guarantor for the manuscript. Funding: None. Competing interests: None stated.
References
|
|
|
![]()