|
|
Case Reports Indian Pediatrics 2002; 39: 83-87 |
||||
|
Burkitt’s Lymphoma Presenting as Acute Budd Chiari Syndrome |
||||
|
M. Issaivanan Suman Kochhar* Banani Poddar Jatinder S. Goraya
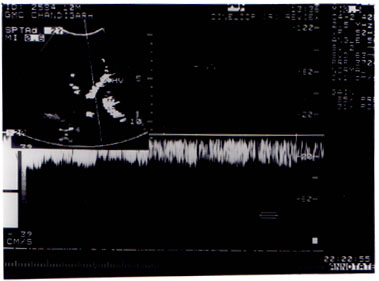
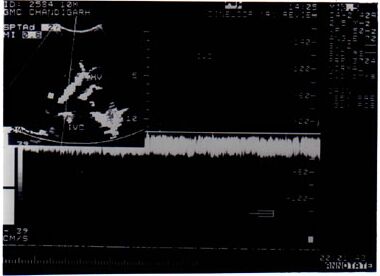
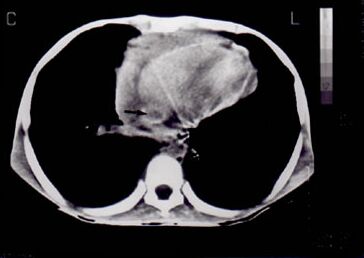
Lymphomas constitute approximately 10% of all childhood cancers being only third in relative frequency after acute leukemias and brain tumors(1). Non-Hodgkin’s lym-phoma constitutes around 60% of childhood lymphomas and its clinical presentation in children is varied depending on the histologic subtype, the extent and the primary site of the tumor(1). Children typically have extra-nodal disease involving the mediastinum (26%), head and neck (29%) or abdomen (31%)(1). Sporadic cases of Burkitt’s lymphoma typically involve the abdomen or head and neck, whereas the endemic type presents as a jaw mass. Acute Budd-Chiari syndrome(BCS) is uncommon in children, with chronic presentation proportionately more frequent than in adults(2,3). This may reflect a more effective establishment of collateral channels or a more vigorous recanalization process at a younger age(2). The association between BCS with lymphomas has been reported only once(5) and Burkitt’s lymphoma presenting as acute BCS has not been reported. We report a child with Burkitt’s lymphoma who presented with clinical and laboratory features suggestive of acute BCS. Case Report A 10-year-old boy was hospitalized with a 15 day history of progressive abdominal distension, abdominal pain and vomiting. Prior to hospitalization he underwent abdomi-nal paracentesis thrice for his abdominal distension draining a total of about 3 liters of ascitic fluid. At admission he was afebrile and had mild pallor with bilateral axillary (1.5 cm) and inguinal (2 cm) lymphadenopathy. He had a heart rate of 100/min, respiratory rate of 24/min, blood pressure of 110/70 mm Hg and a normal jugular venous pressure. Systemic examination revealed a uniformly distended abdomen with dilated anterior and posterior abdominal wall veins with flow from below upwards. He had tense ascites, but no palp-able mass or organomegaly was appreciable. Investigations revealed hemoglobin of 10.5 g/dl; leukocyte count of 18,600 cells/ cumm with 88% neutrophils, 11% lymphocytes and 1% monocytes and platelets of 2.6 × 105/cu mm. His liver function tests showed normal serum bilirubin and alkaline phosphatase levels with elevated alanine and aspartate aminiotransferases (AST/ALT - 107/180 IU). His total serum proteins were 5.2 g/dl with albumin 3 g/dl. The serum electrolytes and renal function tests were within normal limits (Na+136 meq/L, K+4.8 meq/L, urea 24 mg/dl; creatinine 0.1 mg/dl). His serum uric acid was 3 mg/dl and ascitic fluid examination showed 5200 cells with 93% polymorphonuclear neutrophils, protein 6 g/dl, sugar 26 mg/dl and yielded no organism. Malignant cells with morphology suggestive of Burkitt’s lym-phoma were present in the ascitic fluid. Ultra-sonogram (USG) abdomen showed hepato-megaly, ascites, bilateral pleural effusions, well-defined target lesions in the liver with matted bowel loops and a few small upper retroperitoneal lymph nodes. Color doppler studies revealed obstruction of hepatic veins with loss of normal triphasic flow pattern with flow reversal (Fig. 1) and the inferior vena cava (IVC) showed narrowing near the open-ing of hepatic veins with flow reversal (Fig. 2). Computed tomography (CT) scan abdomen showed target lesions in the liver, intraluminal obstruction of the supra-hepatic and intra-hepatic portions of the IVC (Fig. 3) with thickening of bowel wall and diffuse luminal narrowing of intestines. Lymph node biopsy showed high grade non-Hodgkin’s lymphoma consistent with Burkitt’s lym-phoma. Bone marrow biopsy did not show any evidence of infiltration [Clinical staging IV-B, Ann Arbor]. Patient was started on chemotherapy with Cyclophosphamide, Doxorubicin, Vin-cristine and Prednisolone, but he succumbed to his illness on the second day of therapy. Discussion Budd-Chiari syndrome is less common in children than in adults(2,3). In a series of 177 cases by Dilawari et al. only 5% were below 12 years of age(2). Budd-Chiari syndrome is clinically suspected if the triad of ascites, hepatomegaly and right upper quadrant abdominal pain is present. Since this condition is uncommon in children, a high index of suspicion is required to conduct the appropriate studies. The diagnosis depends on appropriate radiological imaging and liver biopsy; hepatic USG concentrating on the hepatic veins combined with doppler flow studies usually confirms the diagnosis. CT scan and magnetic resonance imaging may contribute to the diagnosis but hepatic veno-graphy is the gold standard for diagnosing Budd-Chiari syndrome(4). Various etiologies ranging from idiopathic membranes(2), neoplasias(2), infection(6), trauma(7) and total parenteral nutrition(8) have been described. Although thrombosis associated with an underlying myelo-proliferative disorder is the commonest cause in adults(4), membranous obstruction of inferior vena cava is reported to be the commonest cause in children(9,10). To the best of our knowledge this is the first reported case of BCS associated with Burkitt’s lym-phoma in children (Medlars search, 1980-1999). McDermott et al.(4) reported two adult cases of BCS with myeloproliferative disease progressing on to lymphoma and death. In chronic myeloproliferative disorders, increased viscosity, low grade disseminated intravascular coagulation and active fibrino-lysis, combined with deficiency of liver derived antiplasmin may be contributory to the localization of thrombosis in the hepatic veins(4).
Various treatment protocols have been proposed based on the etiology, the region and the extent of obstruction of the hepatic veins and IVC(2-4). Therapy aims at halting progressive liver damage, with management of the etiologic disorder. Orthotopic liver transplant is the treatment of choice if irrevocable liver damage has occurred. As reported by McDermott et al.(5) in the only two adult cases of BCS with lymphoma, the outcome was fatal as also in our case. Contributors: MI, JG and BP diagnosed and managed the patient, MI and BP conceived the idea and drafted the paper. JG analysed the paper critically. SK worked up the patient radiologically and confirmed the diagnosis and helped in drafting the paper. BP will act as the guarantor for the manuscript. Funding: None. Competing interests: None stated.
References
|
|
|
![]()