|
|
Brief Reports Indian Pediatrics 2002; 39: 70-74 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Prevalence of Tuberculosis Infection in Children Below Fourteen Years in Rural Haryana |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
D. Pattanaik K.B. Singh Guresh K. K. Anand S. Kant S.K. Kapoor
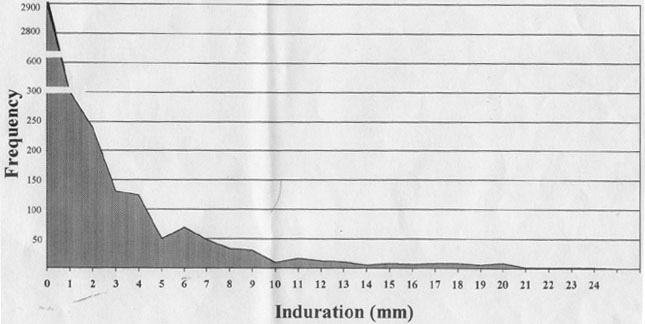
Tuberculosis continues to be a public health problem in India. About 14 million population are estimated to be suffering from active tuberculosis of whom 3-3.5 million are infectious(1). Emergence of Human Immunodeficiency Virus (HIV) infection and multi drug resistant tuberculosis has added an urgency to the situation. Realizing this, India has launched a Revised National Tuberculosis Control Program (RNTCP) which includes the Directly Observed Treatment Short Course (DOTS)(1). A sensitive indicator to assess the impact of a control program is to measure the prevalence of tuberculous infection among children. This is better than the disease status, as it reflects the current rate of transmission of infection rather than infections acquired in the past. The World Health Organization (WHO) has defined tuberculosis control as prevalence of <1% infection in children below 14 years of age. Most of the community based studies on tuberculous infection have been from South India(2,3,4) and are decades old. We, therefore studied, the prevalence of tuberculous infection in children below fourteen years of age in two villages of Faridabad District. District Faridabad has introduced the RNTCP from April 2000. This survey should serve as a baseline prevalence to assess the impact of control after the implementation of the program. Subjects and Methods This study was done in two villages (Dayalpur and Chhainsa) of the Compre-hensive Rural Health Services Project (CRHSP), Ballabgarh which is the rural area adopted by All India Institute of Medical Sciences, New Delhi. The two villages were chosen purposively as it was easier to make frequent visits by the study team for administering the tuberculin test and reading it after 72 hours. The total estimated popula-tion of the two villages was around 11,500 in 1998. The study period was June 1997 to August 1998. All the demographic and health data of these villages are maintained in electronic database and updated on a monthly basis. The BCG coverage in the study area was consistently above 85% for the last fifteen years with above 95% in the more recent years. The tuberculin testing was done by two of the authors (DP, KBS) by domiciliary visits. All the children below fifteen years of age in the two villages were to be covered. If need, be, one repeat visit was made to the family to locate the children. The Purified Protein Derivative (PPD RD 23- 1TU), manufactured by BCG Vaccine Laboratory, Guindy, Madras was used. The PPD was used at least two months before the mentioned expiry date. A dose of 0.1 ml was injected intradermally on the flexor surface of forearm using a tuberculin syringe with 26 G needle. Attempt was made to read the reaction after 72 hours. If a reading was not taken by 96 hours, that child was not taken up for analysis. The reaction was read as the longest diameter of indurated area around the injection site as determined by gentle touch and measured in milimetre by transparent scale. The definition of tuberculin positivity was taken as an induration of >10 mm(5). The data was entered in to Dbase and analyzed using EPI info software version 6.03. Results Based on the computer database, a total of 4654 children below fourteen years of age were expected to be present. Of these, 4200 (90%) could be covered during the survey. The results of the tuberculin testing among them is shown in Fig. 1. The distribution shows a mode at 0 mm. The antimode is at 10 mm induration. This confirms the cutoff point of 10 mm suggested earlier. The agewise prevalence of tuberculin positivity is shown in Table I. Each age group had approximately 300 children. Absence of any reaction to PPD was 75.4% in the infancy, decreased to a low of 57.5% at nine years of age and then rose to 66.2% among thirteen year old children.The prevalence of tuberculin positivity (>10mm) in children below fourteen years age group was 2.4%. (95% CI: 2.1-3.1). There was no significant difference between the two sexes (2.3% among boys and 2.4% among girls). The tuberculin positivity ranged between 0.3% to 2.0% during the under five age group. In the next five year age group, it rose to vary between 1.4% to 5%. In the age group of 10-14 years tuberculin positivity varied from 2.6% to 4.6%.
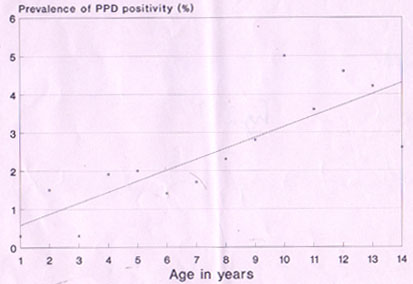
Fig. 1. Distribution of induration following tuberculin testing in children below fourteen years. The age wise prevalence of tuberculin positivity was plotted as a scatter diagram (Fig. 2). A trend line was plotted using method of least squares. The slope of the trend line would approximate the incidence of the infection annually. This was estimated as the b-coefficient in the linear regression. This came to 0.3% per year. A comparison of the reaction to tuberculin between the BCG vaccinated and un-vaccinated group could not be done as the BCG vaccination coverage in the area was above 95% for the past five years. Hence, there were very small number of unvacci-nated children in the under five age group.
Discussion The study assessed the prevalence of tuberculous infection in two villages of northern India. The study found the incidence of the infection in the first year of life to be 0.3%, an estimate which was confirmed by the average trend of increase in the preva-lence till the fourteen years of age group. In the study on tuberculosis epidemiology in south India (1961-68), the prevalence of infection (same definition as in this study) over the study period varied between 1% to 2.1% in the 0-4 years age group, 6.4% to 7.9% in the 5-9 year age group and 15.4% to 16.9% in the 10-14 year age group(2). Similar results have been reported by John et al.(3). In the study by Chakroborthy et al. from Bangalore, the prevalence of infection (>20 mm with 1TU based on identification of antimode in the distribution of reaction) increased from 1.21% in the 0-4 year age group to 5.26% in the 5-9 years age group to 9.20% in the 10-14 years aged children. The prevalence in the total group was 4.76%(4). In a study in rural Delhi in late seventies, the prevalence of infection in the 5-15 years age group was 12.6% (10.5% in 5 to 10 years and 15.9% in 10 to 15 years)(6). In a study in Davangere, the prevalence of infection was 9.8% in 1-4 yr, 9.6% in 5-9 yr old and 14.3% in 10-14 yr old. The positivity was higher in the BCG vaccinated group (15.4% compared to 8%)(7). The results from our study show that the prevalence of infection is similar or lower (<2%) as compared to other studies in the underfive age group. But the subsequent rise is much slower. This could be due to similar exposure of underfive children to tuberculosis infection, mainly through household mem-bers. However, the subsequent difference could be due to difference in exposure to environmental mycobacteria. Haryana has the lowest prevalence of leprosy, another mycobacterial disease, in the country(8). This could be an indirect indication that the environmental exposure to mycobacteriae is less in the study area.
We have also reported many children with no (0 mm) reaction to tuberculin despite having received the BCG vaccine. The reasons are not clear. This could be due to poor reactivity to BCG (problem with vaccine or its administration) or waning of immunity. The low tuberculin positivity could also be due to poor quality of PPD or its administration technique. We used PPD from the national reference laboratory and used it well within the expiry period. However, as we did not test its potency in known positive cases, this can not be ruled out. Tuberculosis control is one of the most important priorities for the country. Given BCG’s doubtful role in prevention, currently the only strategy in place for its control is identification and treatment of cases by DOTS approach. Recently, Jacob John has argued for regular monitoring of TB infection load in the country in order to assess the progress towards control. He also has put forward a case for instituting preventive therapy so as to prevent future bacillary cases and thus interrupt transmission. Towards this objective, he emphasized the need for a national consensus as to when and how children should be tested with PPD, reaction at which preventive therapy should be instituted and choice of drugs, dose and duration(9). Thus, measurement of tuberculosis infection is likely to assume importance in the near future. Our study raises the issues related to administration and interpretation of Mantoux testing due to the regional variation in the reposnse. We will thus, need to standardize the procedure of administration, interpretation and the subsequent management based on the test. The choice of cut-off point will need to be debated and may have to be region specific rather than one for the country. Contributors: DP and KBS were responsible for administering and reading tuberculin test, and doing the data entry. GK co-ordinated the data entry and performed the analysis. KA planned the study, supervised data entry, analyzed the data and prepared the draft. SK co-ordinated the data collection and corrected the draft. SKK conceived the study, provided the overall guidance on analysis and draft correction; he will act as the guarantor for the paper. Funding: None. Competing interests: None stated.
References
|
|
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()