|
|
Original Articles Indian Pediatrics 2002; 39: 12-22 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Comparison of Nebulized Adrenaline versus Salbutamol in Wheeze Associated Respiratory Tract Infection in Infants |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
WHEEZING associated with respiratory tract infection (WRTI) is an extremely common problem in children less than two years of age with reported attack rates in the western literature being as high as 11.4 per 100 children in the first year and 6 per 100 children in the second year of life(1). Viral respiratory infection in infants is often associated with small airway obstruc-tion secondary to an inflammatory process and/or spasm of the bronchial musculature. Infants with such symptoms represent a heterogenous population. Bronchiolitis, wheezy bronchitis, infantile asthma and wheeze associated respiratory tract infection (WRTI) are common diagnoses in such infants(2-4). The role of bronchodilators in this set of small children has been shrouded with controversy and there are a lot of contradictory reports regarding the efficacy of bronchodilators in this setting(5-7). Earlier research showed that children below two years did not respond to bronchodilator therapy whereas later studies have shown that beta-2 receptor stimulants like salbutamol have a definite role in the treatment of such conditions in the younger age group(8-10). Of late there has been renewed interest in the role of adrenergic drugs in WRTI(11). One of the issues in the current debate is whether an alpha agonist, either in combination with beta agonist, or even alone, will be as effective as beta-2 agonist used alone due to its added effect on decreasing the inflammatory edema. The little data available so far, reflect that perhaps a non selective agonist which combines both alpha and beta stimulating properties may be a better choice in treating this condition than a selective beta agonist(12). Traditionally recemic epinephrine has been used as a non-selective adrenergic agonist of choice in wheezy infants due to its supposedly fewer side effects than the more active and more readily available natural laevorotatory form of epinephrine. However, there seems to be no pharmacological basis for this belief(13-15). In addition, L-epinephrine is readily available in all countries while racemic epinephrine is not available in countries like India. Even in countries where both forms are available the racemic form is much more expensive(16). So far there have been very few studies that have compared the efficacy of natural epinephrine with salbutamol in treating bronchiolitis in children. Hence, this study was designed with the dual purpose of: (a) ascertaining whether bronchodilators are indeed effective in wheeze associated respiratory tract infection (WRTI) in infants or not; and (b) comparing the efficacy of a nebulized non specific adrenergic agonist (adrenaline) with a nebulized beta-2 specific agonist (salbutamol) for the treatment of the above condition. Subjects and Methods Study Population The study was conducted in children reporting to the Pediatrics Department of a tertiary level hospital in New Delhi between October 1999 and February 2000 – the typical bronchiolitis season in this part of the country. Children between the ages of two months and twenty four months, attending the hospital with the clinical diagnosis of bronchiolitis(17), i.e., children with their first or second episode of respiratory distress associated with wheezing and clinical evidence of viral respiratory illness in the form of temperature ³38ºC and/or coryza, were included. The following exclusion criteria were used: (i) history of two or more episodes of respiratory distress in the past; (ii) the presence of chronic cardiovascular or respiratory conditions like congenital heart disease, lung cysts, etc; (iii) a history of prematurity or mechanical ventilation in the newborn period; (iv) a family history of asthma; (v) children ill enough to require immediate admission, intravenous fluids and injected drugs such as those with altered sensorium or dehydration, heart rate >180/min, respiratory rate >100/min or lethargy or adjudged to be in incipient respiratory failure. No child was included in the study twice. Table I__Wheezing and Retraction Scales of the Respiratory Distress Assessment Instrument(1)
Table II__Clinical Score (Yale Observation Scale)(18)
Each subject, on arrival, was assessed by one of the authors (MSR). The heart rate and respiratory rate were recorded and the severity of illness assessed by using a com-bination of RDAI score (respiratory distress assessment index)(2) and a clinical score (Yale Observation Scale)(18) (Tables I & II). The RDAI score was used because the three variables, wheezing, retractions and respi-ratory rate, seem best to reflect the underlying pathophysiology and are the most frequently used by clinicians for assessing respiratory status, are non-invasive and have good inter-observer agreement(2). All children were empirically divided into mild, moderate and severe disease categories based on the sum of their RDAI and clinical scores. Children with total scores of 7-15, 16-30 and >30 were classified as having mild, moderate and severe disease, respectively. Oxygen satura-tion was measured non invasively using pulse oxymetry, and those with values less than 93% were designated as having significant hypoxia. The children were then randomly assigned to two groups designated as "A" and "B". Children in Group A received 0.1 ml/kg body weight of 1 in 10,000 solution of adrenaline. The drug was mixed with normal saline to make a total volume of 3 ml and was nebulized using oxygen flow of 8 L/min. Group B received salbutamol in a dose of 0.15 mg/kg body weight (minimum dose 1 mg) also nebulized in normal saline to make a total volume of 3 ml using oxygen flow of 8 L/min. Three doses of each drug were given at 20 minute intervals. Pulse oxymetry was done during this period and SpO2 (pulse oxygen saturation) values recorded at the start of the study (SpO2–1) and ten minutes after the first (SpO2–2), second (SpO2–3) and third (SpO2–4) doses of the drug were compared. No other drugs like antibiotics, steroids, intravenous fluids, etc were given during this period. In febrile children temperature was brought down by hydrotherapy alone. Ten minutes after administration of the last dose, respiratory rate, RDAI score, and clinical score were evaluated again to assess the response to therapy. The decision for further management was taken on the basis of this evaluation. Children who showed a sustained decrease in tachypnea and respira-tory distress (wheezing and retractions), and were accepting well orally after an observation period of three hours were sent home on oral medication. Children who did not improve or showed deterioration were admitted for further mangement. Sample size The study was designed to detect a difference of at least 5% in the SpO2 (mean level of oxygen saturation) between the two drugs with alpha (two tailed a) of 0.1 and power (1 – b) of 0.90. The standard deviation for this calcualtion was taken as 8 as determined from the pilot study. This gave a sample size of 44 in each arm of the study. Analysis Data was recorded on a predetermined proforma and analyzed using Epi-info-5, Microstat, Instat and SPSS statistical software employing appropriate statistical tests like Student’s test, Chi square test and proportions test. Results Ninety one children in the age group of two months to two years were included in the study. Sixty five of these (71%) were males and 26 (29%) females. Most of the patients (82 out of 91, i.e., 90%) were between two months to one year and the rest (9 out of 91, i.e., 10%) were older than one year. The mean age of the children was 5.15 months in group A and 5.62 months in Group B. The mean initial heart rates, respiratory rates, RDAI scores, clinical scores and total scores of the two groups were comparable (Table III). The proportion of cases with mild, moderate and severe disease was similar in both groups – 1, 16 and 28, respectively in Group A and 0, 24 and 22, respectively in Group B (p>0.05). Table III__Comparison of Initial and Final Parameters in Both Groups
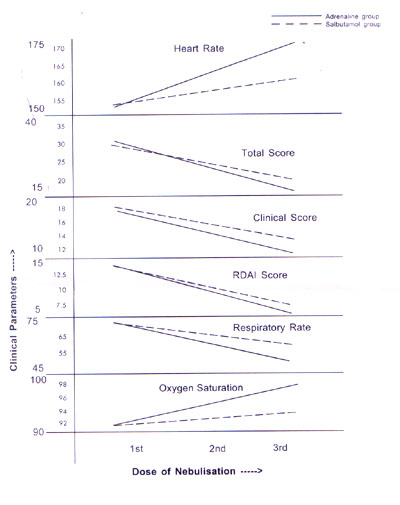
The pulse oxymetry values at the start of the study (Table IV) did not show any significant difference between the two groups. The number of children with significant hypoxia was similar in both groups (19/45 vs 14/46, p = 0.12, Z = 1.16). At the end of the intervention period, i.e., after three doses of nebulization the various study parameters in the two groups were compared with initial values (Table III and Fig. 1). In Group A (adrenaline group), it was seen that the mean respiratory rate had decreased from 73.69 per minute to 52.18 per minute after intervention while the heart rate had increased from 151.89 per minute to 174.64 per minute. The mean RDAI score had fallen from 13.8 to 5.0, the mean clinical score from 18.07 to 10.56 and the total score from 32.24 to 15.56 after therapy (p<0.001 in each case). In Group B, the mean respiratory rate decreased from 73.65 per minute to 60.48 per minute after intervention while the heart rate increased from 152.26 per minute to 160.59 per minute. The RDAI score fell from 13.19 to 7.24, the clinical score from 17.37 to 13.28 and the total score from 30.57 to 20.52 (p<0.001 in each case).
The post intervention values for adrenaline (Group A) and salbutamol (Group B) were compared (Table III). The adrenaline group (Group A) had a significantly lower mean respiratory rate, RDAI score, clinical score and total score as compared to the salbutamol group (Group B) after three doses of nebulization. However, the post-intervention mean heart rate in Group A was significantly higher (Table III). A significantly higher proportion of patients in Group A with moderate and severe distress showed good improvement and converted to normal or mild distress after intervention as compared to Group B (28/44 in Group A vs 12/46 in Group B, p <0.001). The oxygen saturation, measured by pulse oxymeter (Table IV), showed no significant difference between the mean values of the two groups at the start of the study (SpO2–1) and ten minutes after the first dose (SpO2–2). Subsequently, however, there was a signi-ficant improvement in the values recorded after the second and third doses (SpO2–3 and SpO2–4, respectively) of nebulization in both the groups. In the adrenaline group, it increased from a mean value of 90.58 to 98.04, while in the salbutamol group it increased from 91.13 to 93.87 (p <0.001). Also the mean oxygen saturation in the adrenaline group was significantly higher than that of the salbutamol group after the 2nd and 3rd doses. In addition, a greater proportion of patients with significant hypoxia achieved final SpO2 >93% in Group A as compared to Group B (15/19 vs 5/14; p <0.01, Z = 2.512). At the end of the intervention period it was seen that six out of forty five patients in the adrenaline group had either shown no improvement or deteriorated and had to be admitted for further treatment, while the rest could be sent home on oral medication. Correspondingly in the salbutamol group, 14 out of 46 required admission as they failed to respond to therapy (p = 0.02, proportion test).
Fig. 1. Variation in clinical parameters with nebulization. Discussion Respiratory distress due to wheezing is often associated with respiratory tract infection in the first two years of life. It is difficult to make an exact diagnosis in the absence of viral cultures and pathologic findings and usually clinical diagnoses of bronchiolitis, wheezy bronchitis, wheeze associated respiratory infection, etc. are made(17). The main aim of the clinician in such a situation is to provide long lasting relief to respiratory distress by decreasing wheezing and improving air entry. The drug conventionally used for this purpose was nebulized normal saline. Bronchodilators, it was argued, had little role in infants because; (a) there were few smooth muscles in the airways of infants, (b) there was a paucity of adrenergic receptors in the airways, and (c) narrowing of airways was due to bronchiolar debris. However, the last was an autopsy finding from very severe cases and perhaps did not reflect the entire spectrum of the disease. Later, injectable epinephrine was used in wheezing infants with good results(2). Since then, numerous adrenergic agonists, specific and non specific, like salbutamol, metaproterenol, racemic adrenaline, etc. have been used in the nebulized form with mixed results(10,11,19,20) and controversy still remains about the nature, route and dosage of drug to be used. The present study has attempted to verify the efficacy of bronchodilators in WRTI and compare the benefits of a beta-2 specific agonist with a combined alpha and beta (non specific) agonist among children presenting with a first or second episode of wheezing and respiratory distress in association with fever and/or coryza, without any family history of atopy or asthma. So primarily the study was focusing on wheezing in association with RTI, epidemiologically and clinically presumed to be of viral origin and attempts were made to exclude children with atopy. Analysis of results revealed that the children in both the groups had similar clinical profile at the time of inclusion in the study. After three doses of nebulization, both the adrenaline and salbutamol groups showed significant improvement in mean respiratory rate, RDAI score, clinical score as well as oxygen saturation. However, these changes were significantly more marked in the adrenaline group as compared to the sabutamol group for all parameters (p<0.001 for each parameter). Not only were the mean scores and mean SpO2 levels better in the adrenaline group, but also the proportion of patients having significant improvement in clinical scores as well as oxygen saturation were higher in adrenaline as compared to salbutamol group (p <0.01). This benefit in clinicophysiologic profile was also reflected in the need for hospitalization as the admission rate was significantly lower in the adrenaline group (13.3% versus 30.4%; p value = 0.02). Thus, both drugs showed good efficacy with adrenaline being better than salbutamol. The cardiac side effects of drugs used were also assessed because the chronotropic action of adrenergic agents on the heart is often a matter of concern. Both salbutamol as well as adrenaline showed a significant increase in heart rate, more so in the case of adrenaline. However, this had no adverse clinical repercussion like increased irrit-ability, tremors, facial blanching, arrythmia, congestive heart failure and none of the children required drug withdrawl or inter-vention for tachycardia or its consequences. Comparing the study results with the body of research done in the past in this field, certain salient differences, both on terms of methodology and results, emerged. Several of the earlier studies used changes in total pulmonary resistance (TPR) to measure clinical outcome(5,11,21). Yet, experience suggests that TPR may not necessarily reflect on the clinical status(2). With the use of sympathomimetic drugs, if there is a reduc-tion in FRC (functional residual capacity) simultaneously with the amelioration in airway narrowing, there may be no change in measured total resistance despite an improvement in the child’s initial condition. Therefore, the measured changes in TPR may not necessarily correlate with clinical benefits. The problem of objective PFT measurement in small children further limits the use of this modality. Certain authors have used sedation with chloral hydrate(11) before recording PFT in children, but this by itself may affect respiratory status. Therefore in our study, we have instead used a combination of RDAI score and Yale observation scale to assess the respiratory status and degree of distress to the patient. Both these scores are non-invasive, have low inter observer variation and can be easily evaluated in the OPD without the use of complicated equipment. Furthermore, to assess actual physiologic improvement, arterial oxygen saturation by pulse oxymetry was done as some authors have suggested that this may be the best objective criterion to assess degree of distress in children(12). The drug chosen for comparison with salbutamol in the present study (L-adrenaline) is also different from those used by most researchers in the past. The earliest study by Lenney and Milner(11) using both nebulized adrenaline and nebulized phenylephrine, showed no advantage of either drug as compared to placebo, in children with bronchiolitis. However, this study, suffered from many drawbacks. Subsequently, Lowell et al.(2) used injectable epinephrine in wheezy infants and found it to be of benefit. Several studies, thereafter, compared the effects of b2 agonists such as salbutamol with normal saline(10,19,22) in wheezy children and found salbutamol to be more advantageous. More recently, the focus has shifted back to the role of nonspecific adrenergic agonists for their possible effect on reduction of mucosal edema in addition to bronchodilation, thereby possibly providing greater relief than that given by broncho-dilation alone. But most earlier workers have used racemic adrenaline as the non specific adrenegic agent of choice. Kristjansson(12) compared racemic adrenaline with placebo for the treatment of bronchiolitis and concluded that racemic adrenaline was more efficacious. Wennegren et al.(9) in a study of children with wheezy bronchitis, found racemic adrenaline to be more efficacious than nebulized salbutamol. Similarly, Sanchez et al.(21) and Reijonen et al.(23) also found nebulized racemic epinephrine to be better than nebulized salbutamol for the treatment of bronchiolitis. Thus, while several authors have shown that non specific adrenergic agonists are superior to beta-2 specific agonists, almost all of them used racemic adrenaline, the selection of which as the non specific agonist of choice is debatable. There perhaps is no sound pharmacologic basis for the belief that racemic adrenaline is safer than L-adrenaline(13,15). Also racemic adrenaline is not manufactured in India and is thus difficult to obtain and expensive, thus making L-adrenaline a more viable option. To the best of our knowledge there is only one earlier study that has compared L-adrenaline with salbutamol in bronchiolitis(16). In this study, L-adrenaline was found to be more effective though the dose used by the authors (3ml of 1 in 1000 solution per dose) is much higher than in the present study. In view of the reports of facial blanching by nebulized adrenaline reported by them, we decided to use a lower dose (same as the standard subscutaneous dose 0.1 ml/kg 1 in 10,000 solution) for nebulization and found it to be safe and effective. An earlier trial on croupy infants(24) had revealed that the peak effect of nebulized epinephrine appeared in 30 minutes and lasted for 60-90 minutes. In this study, even though the continued effect of the drugs was seen after the third dose, the maximal change in SpO2 appeared in both groups after the second dose of nebulization, i.e., about 30 minutes after the onset of nebulization. This may perhaps explain why certain authors(11) who used only a single dose of adrenergic agonist nebulization did not find it superior to a placebo. In our study too, maximum effect of the drugs was observed after the second dose. In conclusion, it can be inferred that bronchodilators, both specific and non specific are useful in relieving symptoms and improving oxygenation in wheezy infants with clinical diagnosis of WRTI, who present with respiratory distress and wheezing in association with coryza. However, of the two drugs, L-adrenaline shows a better efficacy in terms of relieving distress and improving oxygenation as well as decreasing the need for admission. Larger, multi centric, double blinded randomized controlled trials are required to confirm these results. Contributors: VS designed the study, helped in analysis and drafted the manuscript; he will act as the guarantor for the paper. MSR helped design the study, monitored patients, collected and analyzed the data and co-drafted the manuscript. Funding: None. Competing interests: None stated.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()