K.V. Ramasubramanian
Amit Kumar
S.K. Kabra
V. Seth
From the Department of Pediatrics, All India Institute of Medical Sciences, Ansari Nagar, New Delhi
110 029, India,
Reprint requests: Dr, S.K. Kabra, Associate Professor, Department of Pediatrics, All India Institute of Medical Sciences, Ansari Nagar, New Delhi 110029. India.
The use of antibodies to give passive protection for the severely injured came to the attention of medical persons during the period of second world war. Cohn and his colleagues(1) in 1940 studied the antigen specific immunoprotective properties of the serum which led to the separation of gammaglobulins from serum without damaging their antibody properties.
Initially IgG was formulated for intra-muscular injection. The injections are painful and the amount of IgG that can be given is limited. Absorption after intramuscular injection is slow and erratic due to proteolytic degradation of IgG at the injection' site and it is difficult to maintain serum IgG levels above 2g/L. The risk of a severe adverse reaction is significant, upto 20% of patients have an anaphylactic reaction at some time(2). 10 overcome the aforementioned limitations. of intramuscular preparation, intravenous immunoglobulin (lVIG) was
developed and became popular as purified preparations had relatively fewer side effects.
Mechanisms and Immunomodulatory
Effects
IVIG exhibits immunomodulatory properties that are mediated by the Fc portion of IgG
and by variable (v) regions contained in the immune globulin preparations. These
effects are categorized as early and long-term effects depending on whether they
are
identified during or beyond the half life of IVIG(1,3). Table I depicts the early. effects of IVIG. The long-term effects of IVIG include a complex set of effects that may be observed in individuals receiving IVIG far beyond the half life of the infused IgG. These are mainly observed in patients with autoimmune diseases. Apart from the direct neutralization of autoantibodies, anti-idiotypes in IVIG directed to surface immunoglobulin on B. lymphocytes play an important role in the ability of IVIG to downregulate or stimulate antibody production by B cells(4). Anti-CDS antibodies in IVIG modulate auto-immunity by reacting with CDS+ (B-1) subpopulation of B
cells(5). Similarly, anti-CD4 antibodies in IVIG inhibit the proliferative responses in conventional mixed lymphocyte reaction as well as the in vitro infection of CD4 T cells with HIV-I(6). These observations may be of clinical relevance in situations such as graft versus host disease (GVHD) in recipients of bone marrow allotransplants(7) or in auto- immune diseases. It was also observed that restoration of a normal pattern of spontaneous fluctuations of autoantibody titres (similar to normal physiological states) occurred following IVIG transfusions in patients with autoimmune diseases(8). Thus, the beneficial
effects of IVIG in autoimmune diseases are not merely due to passive transfusion of neutralizing anti-idiotypic antibodies against autoantibodies but also due to IVIG altering the structure and dynamics of the idiotypic network in autoimmune disorders.
TABLE I - Early Effects of IVIG
|
Mechanism |
Example |
|
1.
Neutralization of bacterial toxins and viruses |
- Infections,
Sepsis |
2.
Facilitation of microbial clearaqce
-
enhancement of opsonization
-
stimulation of cell mediated immunity |
- Infections, Sepsis |
|
3.
Synergism with
β -
lactam antibiotics |
- Infections,
Sepsis |
|
4.
Functional blockade of Fc receptors on splenic macrophages |
- ITP |
|
5. Increase in solubility and clearance of immune
complex |
- Vasculitis |
|
6. Neutralization of circulating auto antibodies (Anti-idiotype antibodies) |
- Autoimmune
disorders |
|
7.
Inhibition of complement mediated damage (inhibition of C3b and C4b uptake by target cells) |
- Dermatomyositis |
8.
Modulation of production of proinflammatory cytokines
|
- Inflammatory
condition
i.e., Kawasaki disease |
Pharmacokinetics
The half life of IVIG is 18-23 days in normal individuals; but varies in patients . with antibody deficiency(9). It gets rapidly distributed to the. extravascular space with about half the IgG being redistributed to the extravascular compartment during the first 3 to 5 days after IV infusion(10). Elimination of IVIG occurs through reticuloendothelial system.
Clinical Uses
There are quite a few definite indications of IVIG but it is expected to playa role in many more disorders. The various clinical indications are listed in Table II.
Primary Immunodeficiency
Antibody deficiency states such as
x-linked hypogammaglobulinemia form the most obvious indication for IVIG use(11). IVIG
has reduced the mortality and morbidity from bacterial infections in these disorders(12). Its use may also confer benefit to patients with primary immunodeficiency states like severe combined immunodeficiency, Wiskott-Aldrich syndrome and. ataxia-telangiectasia which do not have antibody deficiency alone( 11).
The aim of IVIG infusion is to maintain trough IgG levels above 5 g/L and this can be achieved in most patients by giving about 0.4
g/kg/month. Sometimes infusion is required at 2 to 3 weekly intervals(13). Liver functions
should be monitored at regular intervals, if possible at every IVIG infusion in order to detect a transmission event(l3). As chronic lung disease is the most common cause of death in these patients( 12) and as chest disease may progress insidiously despite optimal IVIG replacement; review of pulmonary function with full chest ancillary treatment should be instituted at regular intervals(10).
TABLE II - Clinical Uses of IVIG
I. Established Indications
(As evidenced by large
number of trials) |
1.
Antibody deficiency
- Primary
- Secondary (HIV infection) |
| 2.
Immune thrombocytopenic purpura |
| 3.
Kawasaki disease |
| 4.
Guillain Barre Syndrome |
| 5.
Chronic Demyelinating Inflammatory Polyneuropathy (CDIP) |
II. Probable Indications
(Controlled trials are still
needed) |
1. Infections
(i) Bacterial infections
(ii) Viral infections
(iii) Neonatal sepsis |
6. Vasculitis
(i) Wegener's granulomatosis
(ii) Microscopic polyangitis
|
2. Allergic
Diseases
(i) Bronchial asthma
(ii) Atopic dermatitis
|
7. Autoimmune
disorders
(i) SLE
(ii) Autoimmune neutropenia
(iii) Autoimmune hemolytic anemia |
3. Cardivascular
(i) Viral myocardititis
(ii) Acquired cardimyopathy |
8. Endocrine
(i) IDDM
(ii) Grave's disease with opthalmopathy |
4.
Gastrointestinal
(i) Inflammatory bowel disease
|
9.
Miscellaneous
(i) Critically ill patients
(ii) Prophylaxis in bone marrow transplants |
5. Neurological
(i) Multiple sclerosis
(ii) Myasthenia gravis
(iii) Intractable epilepsy |
|
Self infusions of IVIG in the patient's home is a sensible alternative to hospitalization. It is cost effective, more convenient and reduces the chances of nosocomial infections(10). However, selection of the patient is important; they must have received IVIG therapy for 4 to 6 months without side effects; must be well motivated; have a parent or caregiver who should be able to administer IVIG
and recognize and treat adverse reactions, if any(10). Some studies have shown that subcutaneous rapid infusions of gamma-globulin at home provides the same efficacy as home IVIG and IMIG therapy are associated with fewer side-effects(14).
HIV Infection
IVIG therapy in HIV infection has reduced the incidence of serious bacterial infections by 25%(15). However, IVIG therapy has not shown reduction in mortality(15,16). More recently, a large study conducted by the AIDS Clinical Trials Group showed that IVIG does not offer a significant benefit for patients on antiretroviral therapy who are also receiving trimethoprim-sulfamethoxazole prophylaxis for Pneumocystis carinii
pneumonia(16). However, in another study it was shown that the effect of IVIG was independent of trimethoprim-sulfamethaxazole prophylaxis(17). Further studies are necessary to compare the efficacy of cheaper trimethoprim and expensive IVIG in prevention of bacterial infections. Also, whether therapy with IVIG benefits asympomatic HIV infected children or not remains to be answered.
Currently, the use of IVIG should be reserved for children who meet the following criteria(16): hypogammaglobulinemia (IgG <250 mg/dl), recurrent serious bacterial infections, thrombocytopenia (platelets <20000Icumm), two or more episodes of pneumonia, absence of antibody formation, chronic bronchiectasis and lack of measles antibody while living in an endemic area. The usual dose is 0.4 g/kg administered every 4 weeks( 16).
Kawasaki Disease
The therapy for Kawasaki disease is aimed at reducing inflammation in the coronary arterial wall and myocardium. IVIG reduces endothelial inflammation through inhibition of cytokine production and' anti- endothelial antibodies and also neutralization of toxins(18).
It has been reported that IVIG plus aspirin cause a pronounced resolution of inflammation, significant reduction in coronary artery abnormalities, rapid resolution of fever and normalisation of laboratory parameters as compared to aspirin alone(18,19). IVIG
therapy results in a reduced prevalence of giant aneurysm and accelerates normalization
of abnormalities of left ventricular systolic function and contractility too(20). IVIG is currently recommended during acute stage of Kawasaki disease in the dose of 2 g/kg as single infusion over 12 hours (preferred) or IVIG 0.4 g/kg per day for 5 days(19).
There are some unresolved therapeutic issues(19,20). First, there are no controlled trials for assessing the efficacy of IVIG in patients appearing after the tenth day of
.
fever. However, most clinicians prefer to treat these patients with IVIG if they are still febrile or if they have coronary artery disease. Second, there is a group of patients who fail to respond or continue to have fever despite IVIG therapy, as prolonged fever is associated with increased risk of coronary abnormalities. Re-treatment with IVIG should be considered in these situations though the benefits of treatment in the prevention of coronary arterial abnormalities have not been determined. Third, some 'patients who present within 10 days of onset of illness already have coronary artery abnormalities. Standard therapy should be given to them though there are no data available on the acute or long term benefits of such therapy. Finally, despite IVIG therapy, 6-10% of children will develop. coronary arterial abnormalities(18-20).
Immune Thrombocytopenic Purpura (ITP)
Childhood ITP is an acute, self limited disorder with spontaneous recovery in 90% of cases(21). So conservative management is indicated for majority of children. The major reason to initiate treatment in severely thrombocytopenic children is to prevent intra-cranial hemorrhage or life threatening hemorrhage. However, intracranial. hemorrhage is a rare complication (seen in children with platelet counts <20000/cumm(22,23). Steroids and IVIG shorten the period of severe thrombocytopenia but do not affect the duration of disease(21). Therefore, they are usually reserved for children with persistent thrombocytopenia
<20,000/cumm), especially for those having significant bleeding(21 ,22).
IVIG has become the treatment of choice for producing a rapid increase in platelet counts(22,23). It also showed long term improvement in some patients with chronic lTP without any further treatment(23). The advantages of IVIG include its lack of toxicity, its high rates of efficacy" and possibility of curative effects(24). The main disadvantage is its high cost. The usual dose is
1 g/kg/day for 2 days or 0.4 g/kg/day for 5 days. For severely affected child with life threatening hemorrhage a combination of IVIG and
intravenous methylprednisolone may be synergistic(25).
Guillain-Barre Syndrome (GBS)
GBS is a self limited disease with a good prognosis for most children. However, approximately 10-20% of children develop respiratory failure and require mechanical ventilation(26,27). Approximately 10-15% may have permanent neurological deficits(28). It is for these children that the specific treatment modalities have been applied.
Plasmapheresis is the first specific treatment that has been proved
to
be effective, if applied early(26,29). Morbidity is decreased and outcome improved. Moreover, time spent on ventilation is shortened. However, plasmapheresis
is a cumbersome procedure and it has its own disadvantages(26,27); it is
difficult to perform because of difficult vascular access in children. Volume overload or hypotensive episodes may complicate the procedure and co-medication is removed
jointly with the unknown adverse disease. factors. Moreover, there are no randomized controlled plasma exchange trials in children with GBS.
The Dutch Guillain-Barre Study Group demonstrated that high dose IVIG is at least as effective as plasmapheresis and possibly more effective if given early(30). In that study the use of IVIG shortened the time to recover independent locomotion, decreased'
the mean duration of artificial ventilation and ,lessened. the complication rate in comparison with plasmapheresis. More recently plasma exchange/sandoglobulin Guillian Barre syndrome trial group studied adult patients with GBS and found that IVIG
and plasmapheresis had equivalent efficacy especially during the first two weeks after onset of neurological syndromes(31). They also noticed that combination of plasmapheresis with IVrG
did not provide a significant advantage except the reduction of
disability grade after 4 weeks was just significant in favor of
combined regimen than with either treatment alone. Also, IVIG can be given safely to children including those with autonomic instability at less cost than plasmapheresis(26). The dose usually used is 0.4-1 g/kg/day for 2-5 days(32). Until randomized controlled trials are reported for pediatric population, IVIG is the preferred treatment for children with acute GBS and rapid neurological deterioration(26) and it should be given early in the course. However, about a quarter of IVIG treated patients and a third of plasmapheresis treated patients will continue to deteriorate in the first two weeks during treatment even if therapy started early(27). Therefore, there is need of more effective therapy. One pilot study conducted by Dutch Study Group demonstrated that combination of IVIG
and high dose Methylprednisolone may be synergistic(33). However, these results need confirmation in a randomized controlled trial.
Chronic Inflammatory Demyelinating Polyneuropathy (CIDP)
The management of CIDP is identical to that of GBS. But unlike in GBS, corticoster- oids have been reported to be beneficial both in children and adults(34,35). Though it is a cheap and
effective form of therapy, the long-term use of steroids is likely to cause serious side effects(26). Plasmapheresis also has been proven useful in CIDP in adults(36). However, it has its own limitations for use in children as already discussed.
IVIG therapy is shown to be effective in CIDP patients. The usual dose is 0.4- I g/kg/ day for 5 consecutive days. If patient deteriorates, intermittent IVIG infusion can be given. The proportion of patients with CIDP responding to IVIG has been variable. The characteristics of responders haye not been defined. In addition IVIG therapy does not prevent relapses, nor does it prolong the duration of remission though it causes rapid l;ecovery(26). IVIG may still have a place as other therapeutic modalities have limitations and significant side effects.
Refractory Dermatomyositis
Corticosteroids are the mainstay of therapy for dermatomyositis. They are required
to be continued for the minimum of 2 years(37). Majority of the
patients seen in
early course do well with this standard therapy. However, adjunctive therapy is necessary
for some patients(37) including those with severe onset, a relapsing course. or a chronic persisting course. Azathioprine, methotrexate and cyclo-sporin have all peen reported to be beneficial in these patients. Unfortunately, all these drugs are associated with potential immunosuppressive side
effects. As IVIG has immunomodulatory effects with minimal side effects, it also has been tried in such refractory patients. It has been reported that IVIG is a safe and effective treatment for refractory dermatomyositis(38,39). These studies suggested that the clinical response to IVIG is often rapid, and corticosteroid dose may be reduced in most. patients. However, efficacy of IVIG is short lived even repeated courses may prove inadequate(38).
Bone Marrow Transplantation (BMT)
The major complications of allogenic bone marrow transplantation are graft rejection, graft versus host disease (acute or chronic) and opportunistic infections. Immunosuppressive drugs (steroids, cyclosporin) have greatly reduced the morbidity and mortality by reducing the first two of the three complications but they are not without their side effects including the increased. risk of opportunistic infections.
SuIIivan et al.(7) found that weekly ad- ministration of IVIG (500 mg/kg) up to day 90 after transplant had a significant reduction in frequency of acute GVHD, interstitial pneumonia and infection. A recent meta analysis of 12 randomized trials of IVIG pro- phylaxis in bone marrow transplants revealed a significant reduction in fatal CMV infection, CMV pneumonia, non-CMV interstitial pneumonia and acute GVHD
in patients receiving IVIG prophylaxis(40). As dose schedule and duration of IVIG prophylaxis varied widely in prior studies, further studies need to be conducted to determine the place of IVIG in prevention of certain complications
following BMT.
Neonatal Infection
Preterm babies may have antibody deficiency due to inadequate transfer of maternal antibodies. Endagenous production
of antibodies does not begin till 24 weeks after birth. These factors may make neanates especially preterm babies vulnerable to. infection and sepsis.
IVIG appears to. have a role in sepsis as it neutralizes bacterial toxins, enhances
opsonisation and chemotaxis and modulates cytokine release. Several studies were can- ducted to. demonstrate the efficacy
of IVIG in the prevention and treatment of neonatal sepsis. A recent meta-analysis
of these studies( 41) showed that there was no significant reduction in morbidity and mortality from sepsis in the IVIG treated group compared to. the placebo. group. In addition the therapeutic efficacy
of IVIG in sepsis in very law birth
weight and extreme premature infants is not
clear. Currently, there is no clear evidence far the use of IVIG in prophylaxis
and treatment of neonatal sepsis.
Apart from its doubtful role, IVIG has certain limitations. First, benefit will
occuronly if the IVIG lot contains antibodies to the offending pathogens. So, IVIG preparations
or monoclonal antibodies that possess specific antibodies to key neonatal pathogens may be effective. Second, there is a probable risk
of delayed blockade of reticuloendothelial system. These issues remain to be answered.
Miscellaneous
Though the number of conditions that benefit from IVIG therapy is never ending, it is worth remembering same
of the following indications. In systemic lupus erythematosus, the primary indication for IVIG therapy is severe lupus-associated thrambacytapenia(42). However, relapses are frequent which may
occur either during or after IVIG therapy. Hence, IVIG is mainly used as a short-term approach to prepare the patient far surgery or
to control acute severe bleeding. IVIG can also be used far well selected cases
of lupus nephritis such as patients with active membranous glomerulonephritis unresponsive to conventional treatment
or where renal function is preserved or only mildly compromised(43).
Based an the evidence of IVIG use in Kawasaki's disease, a retrospective study was conducted which found that children with acute myacarditis treated with IVIG had shown an improved recovery
of left ventricular function and enhanced first year survival as compared to controls(44). However, prospective randomized trials arc needed to define the exact role. The indication for IVIG
therapy in myasthenia gravis are the same as those for plasmapheresis to provide short-term benefit in any patient with sudden
worsening of myasthenic weakness, or prior to. surgery( 45). The usual
dose is 400 mg/kg/ day far five consecutive days. The benefit may be substantial in an individual patient; however, it varies from patient to. patient.
IVIG is an attractive treatment option in autoimmune hemolytic anemia because of its ability to. induce patent blockade
of reticulondathelial system. However only one third of patients respond to
this therapy( 46). In addition, higher doses are required (1 g/kg/day far 5 days). Thus, IVIG is not a standard treatment, but it can be tried in patients who. are refractory to steroid therapy.
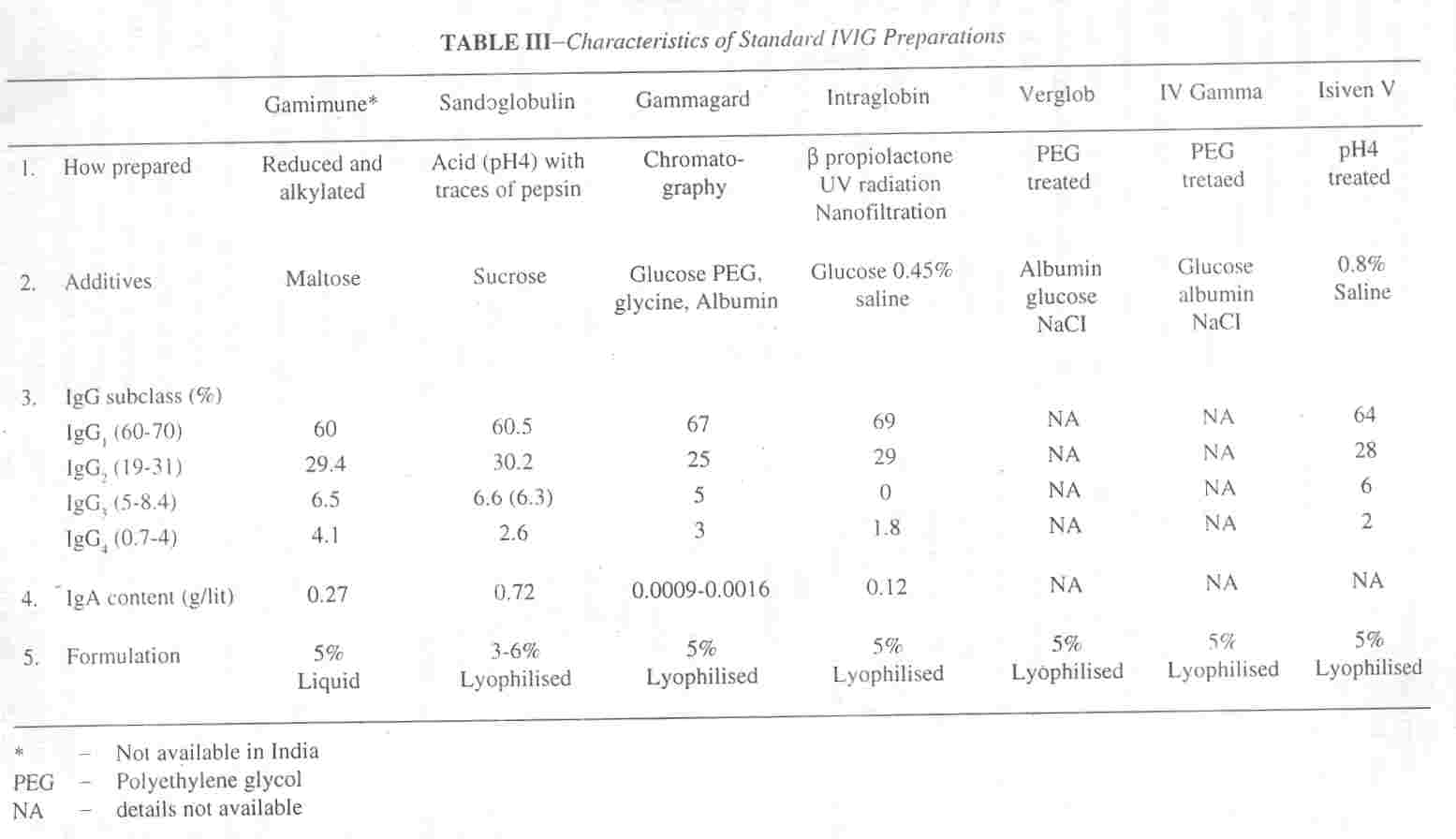
Characteristics of IVIG Preparations
IVIG preparations are same of the safest biological products available. To. minimize the side effects. WHO recommended certain standards for manufacturing IVIG preparations(47)-each lat should be derived from plasma pooled from at least 1000 donors; it should contain at least 90% intact IgG, with' the subclass present in normal ratios; it's IgG molecules should maintain biological activity such as complement fixation; and it should be free of IgG aggregates, prekallikrein activators and infectious agents.
To meet the above criteria, most manufacturers use cold ethanol fractionation technique followed by one of a variety of procedures. The properties of various IVIG preparations are mentioned in Table lII(48- 50). Among them, the preparation treated at pH 4, the albumin protected product and the chemically modified preparations (e.g.,
β- propiolactone) are essentially intact and free of harmful contaminants. Several treatments such as solvent detergent technique, gamma- radiation, and pasteurisation are under trial to render IVIG free of viral contaminants. Additives are used to increase the solubility and stability of IgG molecule, IgG subclass distribution in a standard IVIG preparation should be similar to that of plasma. Intraglobin which is devoid of IgG3 may not be ideal in this respect.
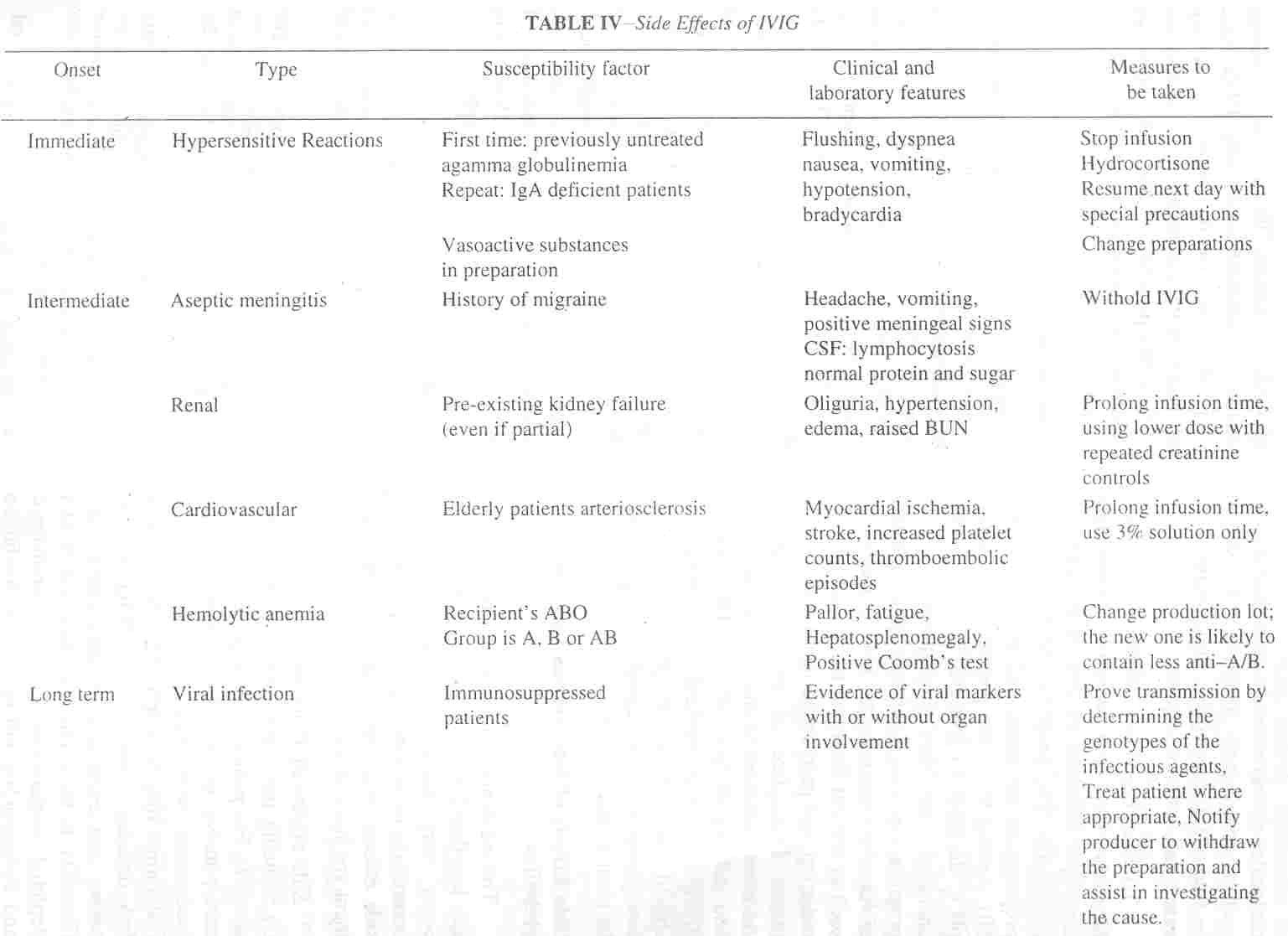
Side Effects of Intravenous Immunoglobulins
The incidence of adverse reactions is usually less than 5%(51). Most of these
reactions occur very rarely and usually. do not contraindicate
further therapy. The variety of side effects, risk factors and
their management are listed in Table IV(52).
Side effects of IVIG are often alleviated by reducing the rate or the volume of infusion(51). For patients with repeated reactions unresponsive to the above measures, pre-medication
with hydrocortisone or anti-histaminics may be helpful(52). Patients with IgA deficiency who recieve IVIG
develop
severe and even fatal anaphylactoid reactions(53). In those rare instances, use of IgA depleted preparations such as Gammagard and Polygam(50) will reduce the likelihood
of further reactions. Ideally, these patients should be screened before any IVIG
infusion. However, routine screening is not necessary as the combination of the absence of IgA and presence of anti-IgA antibodies required for precipitating reaction is infrequent(51).
Conclusions
IVIG, a novel immunomodulatory agent has a promising role in various disease states. Its mechanism of action include direct neturalisation
of antigens and toxins, blockade of Fc receptors, suppression of synthesis of cytokines and autoantibodies and modulation
of immunological network. Though its clinical uses are
innumerable, the current definitive indications include primary immuno-deficiency, ITP, Kawasaki disease, GBS and CDIP. The main advantages of IVIG therapy are its fewer side effects and ease of administration. The limitations include high cost of therapy, possible risk of transmission of infectious agents and serious anaphylactic reactions especially in patients with IgA deficiency. Fortunately, the availability of newer preparations will render IVIG more effective and free from these limitations.
|
1.
Dwyer 1M. Immunogobulins in autoi- mmunity: History and mechanisms of action. Clin Exp Rheumatol 1996; 14 (Suppl 15): S3-S7.
2.
Hill LE, Moltison PL. Hypogammaglobulinemia in the United Kingdom. 13. Conclusions. Medical Research Council Special Report Series No. 31, London, 1971; pp 124- 127.
3.
Kaveri SV. Mouthon L, Kazatchkine MD. Immunomodulating effects of intravenous immunoglobulin in autoimmune and inflammatory diseases. 1 Neural Neurasurg Psychiatry 1994; 57: S6-S8.
4.
Mouthon L. Kaveri
SV,
Spatter SH,
Desmazes L, Lefranc C, Desai R, et al. Mechanism of action of IVIG in immune-me- diated diseases. Clin Exp Immunol 1996; 104 (Suppl I): 3-9.
5.
Vassilev T. Gelin C, Kaveri SV. Zilber MT, Boumsell L. Kazatchkine DM. et al. Antibodies to the CD5 molecule in normal human immunoglobulins for therapeutic use. Clin Exp Immunol 1993: 92: 369-372.
6.
Hurez V, Kaveri SV, Mouthob A, Dietrich G. Mani JC, Klatzmann D, et al. Anti CD4 activity of normal human immunoglobulins for therapeutic use (lVIG). Therap Immunol 1994; I: 269-278.
7.
Sullivan KM, Kopecky Kg, Jocom J, Fisher L. Buckner CD. Meyers DJ, et al. Immunomodulatory and anti-microbial efficacy of intravenous immunoglobulin in bone marrow transplantation. N Engl J Med 1990: 323: 705-709.
8.
Dietrich G, Varela F, Hurez V, Bounamin M. Kazatchkine MD. Selection of the expressed B cell repertoire by infusion of normal immunoglobulin G in a patient with autoimmune thyroiditis. Eur J Immunol 1993; 23: 2945- 2950.
9.
Mankarious S. Lee M, Fisher S, Pyun KH, Ochs HD, Oxelins VA. et al. The half lives of IgG
subclasses and specific antibodies in patients with primary immunodeficiency who are receiving intravenously administered immunoglobulin. J Lab Clin Med 1988; 112: 634-640.
10.
Hayney M. Intravenous immune globulin in primary immunodeficiency. Clin Exp Immunol1994; 97 (Suppl1): 11-15.
11.
WHO Scientitic Group. Primary immunodeficiency diseases. Immunodeficiency Rev 1992; 3: 195-236.
12.
Hermaszewski RA, Webster ADB. Primary hypogammaglobulinemia: A survey of clinical manifestations and complications. Quart J Med 1993; 86: 31-42.
13.
Chapel HM. Consensus panel for the diagnosis and management of primary antibody deficiencies.
Consensus on diagnosis and management of primary antibody deficiencies. Br Med J 1994: 308: 581-585.
14.
Gardulf A. Hammarstorm L, Smith CIE. Home treatment of hypogammaglobulinemia with subcutaneous immunoglobulin by rapid infusion. Lancet 1991: 338: 162-166.
15.
Jenkins M. Human immunodeficiency virus
type I infection in infants and children.
1/1:
Rudolph's Pediatrics, 20th edn. Eds. Rudolph AM. Hoffman HE. Rudolph CD. Connecticut; Appleton and Lange 1996; pp 660-661.
16.
Delia M, Hernandez R. Scott GB. HIV infection.
1/1:
Gellins and Kagan's Current Pediatric Therapy. 15th edn. Eds. Burg FD, Ingelfinger JR, Wald ER, Polkin RA. Philadelphia. W.B. Saunders Co. 1996; pp 645- 651.
17.
Mofenson M, John. Moye JR, Korelitz J, Bethel J, Hirschhorn R. Nugent R. et al. Cross over of placebo patients to intravenous immunoglobulin confirms the efficacy for prophylaxis of bacterial infections and reduction of hospitalization in human immunodeficiency virus-infected children. Pediatr Infect Dis J 1994; 13: 477-484.
18.
Leung DYM. Kawasaki Syndrome: Immunomodulatory benefit and potential toxin neutralization by intravenous immunoglobulin. Clin Exp Immunol 1996; 104 (Suppl I): 49-54.
19.
Dajani AS. Taubert KA. Gerber MA. Shulman ST. Ferrieri P. Freed M, et al. Diagnosis and therapy of Kawasaki disease in children. Circulation 1993: 87: 1776-1780.
20.
Sundel RP. Newberger JW. Kawasaki Syndrome. 1/1: Gellins and Kagan's
Current Pediatric Therapy, 15th edn. Eds. Burg FD. Ingeltingcr JR. Wald ER, Polkin RA. Philadelphia. W.B. Saunders. Co. 1996; pp 195-197.
21.
Manco-Johnson MJ. Hemostasis and Bleeding
Disorders.
111:
Rudolph's Pediatrics, 20th edn.
Eds. Rudolph AM, Hoffman JIE, Rudolph CD. Connecticut. Appleton and Lange. 1'996; pp 1241-1242.
22. Blanchette VS. Luke B,
Andrew M, Sommerville-Nielsen S, Barnard D, Barrie D Veber, et al. A prospective randomized trial of high-dose intravenous immune globulin g therapy, oral prednisone therapy and no therapy in childhood acute immune thrombocytopenic purpura. J Pediatr 1993; 123: 989-995.
23.
Imbach p, Wagner HP, Berchtold W, Gaedicke G, Hirt A, Joller P, et al. Intravenous immunoglobulin versus oral corticosteroids in acute immune thrombocytopenic purpura in childhood. Lancet 1985; ii: 464- 468.
24.
Bussel JB, Goldman A, Imbach P. Schulman I, Hilgartner MW. Treatment of acute ITP in childhood with intravenous infusion of gammaglobulin. J Pediatr 1985; 106: 886- 890.
25.
Hara T, Sochida Miyazaki N, Goya N. High dose gammaglobulin and methylprednisolone therapy for idiopathic thrombocytopenic purpura in children. Eur J Pediatr 1985; 144: 240-242.
26.
Haslam RHA. The polyradiculopathies 111: Gellins and Kagan's Current Pediatric Therapy, 15th edn. Eds. Burg FD, Ingelfinger JR, Wald ER, Polkin RA. Philadelphia, W.B. Saunders Co, 1996; pp 71-73.
27.
Vander Meche FGA. The Guillain-Barre Syndrome: Plasma exchange or immunoglobulins intravenously. J Neurol Nerosurg Psychiatry 1994; 57 (Suppl): 33-34.
28.
Ouvrier R, Rapin I. Childhood neuropathies. 111: Rudolph's Pediatrics, 20th edn. Eds. Rudolph AM, Hoffman JIE, Rudolph CD. Connecticut Appleton and Lange, 1996; p 1972.
29.
French Co-operative Group on Plasma Exchange in Guillain-Barre Syndrome. Efficacy of plasma exchange in Guillain-Barre syndrome: Role of replacement therapies. Ann Neuro11987; 22: 753-761.
30.
Van Der Meche FGA, Schmitz PIM, Dutch Guillain-Barre Study Group. A randomized controlled trial comparing intravenous immunoglobulin and plasma exchange in Guillain-barre syndrome. N Eng J Med 1992; 326: 1123-1129.
31.
Plasma Exchange/Sandoglobulin Guillain-Barre\Syndrome Trial Group. Randomized
trial of plasma exchange, intravenous immu- noglobulin and combined treatment in Guillain-Barre Syndrome. Lancet 1997; 349: 225-230.
32.
Shahar E, Murphy EG, Roifman CM. Benefit of intravenously administered immune serum globulin in patients with Guillain-Barre Syndrome. J Pediatr 1990; 116: 141-144.
33.
The Dutch Guillain-Barre Study Group. Treatment of Guillain-Barre syndrome with high dose immuneglobulins combined with methyl prednisolone: A pilot study. Ann Neurol 1994; 35: 749-752.
34.
Dyck PJ, O'Brien PC, Oviatt KF, Dinapoli RP, Doube JR, Bartleson JD, et al. Prednisone improves chronic intiammatory demyelinating polyneuropathy more than no treatment. Ann Neurol 1982; 11: 136-141.
35.
A Van Doorn PA. Intravenous immuneglobulin treatment in patients with chronic int1ammatory demyelinating polyneuropathy. J Neurol Neurosurg Psychiatry 1994; 57 (Suppl): 38-42.
36.
Dyck PJ, Daube J, O'Brien PC, Pineda A, Low PA, Windebank AJ, et al. Plasma exchange in chronic int1ammatory demyelinating polyneuropathy. N Engl J Med 1986; 314: 461-465.
37.
Miller LC, Tucker LB, Schaller JG. Dermatomyositis and polymyositis. In: Gellins and Kagan's Current Pediatric Therapy. 15th edn. Eds. Burg FD, Ingelfinger JR, Wald ER, Polkin RA, Philadelphia. W.B. Saunders Co, 1996; pp 386-387.
38.
Cherin P, Herson S, Wechsler S, Piette J, Bletry 0, Coutellier A, et al.
Efficacy of intravenous gammaglobulin therapy in chronic
refractory polymyositis and derrnamyositis: An open study with 20 adult patients. Am J Med 1991; 91: 162-168.
39.
Dalakas M. illa I, Dambrosia JM, Soveidan AS, stein PD. Otero C. et al. A
controlled trial of high dose intravenous immunoglobulin in-
fusion as treatment for dermamyositis. N Engl 1 Med 1993; 329: 1993-2000.
40.
Bass EB, Powe NR, Goodmann SN, Graziano SL, Griffiths RI, Kichler TS, et al. Efficacy of immune globulin in preventing complications of bone marrow transplantation: A meta "analysis. Bone Marrow Transplant 1993; 12: 273-282.
41.
Lacy JB, Ohlson A. Administration of intravenous immunoglobulins for prophylaxis or treatment of infection in preterm infants: Meta-analysis. Arch Dis Child 1995; 72: F151-F155.
42.
Maier WP, Gordon DS, Howard RF, Soleb MN, Miller SB, Liberman ID, et al. Intravenous immunoglobulin therapy in systemic lupus erythematoses-associated thrombocytopenia. Arthritis Rheum 1990; 33: 1233- 1239.
43.
Palla R, Cirami C. Bionda A, Marchitiello M. High dose intravenous gammaglobulin for membraneous nephropathy. Clin Nephrol 1986; 26: 314.
44.
Drucker NA, Colan SD, Lewis AB, Bieser AS, Wessel DL, Takahashi AM, et al. y- Globulin treatment of acute myocarditis in the pediatric population. Circulation 1994; 89: 252-257.
45.
Gajdos P. Intravenous immunoglobulin in myasthenia gravis. Clin Exp Immunol 1994; 97: S45-S51.
46.
Bussel JB, Cunnigham-Rundler C, Abraham
C. Intravenous treatment of autoimmune" hemolytic anemia with very high dose of gammaglobulin. Vox Sang 1986; 51: 264- 269.
47.
IUIS/WHO Report. Appropriate uses of human immunoglobulin in clinical practice: Memorandum from an lUIS/WHO
meeting. Bull World Health Organ 1982: 60: 43-47.
48.
Weisman LE. The safety of intravenous immunoglobulin preparations: Isr J Med Sci 1994; 30: 459-463.
49.
Roomer J, Morgenthaler 11 Scherz R, Skvaril F. Characterization of various immunoglobulin preparations for intravenous application. Vox Sang 1982; 42: 62-73.
50.
Taketoma CK, Hodding JH, Kraus DM. Immune Globulin intravenous. III: Pediatric Dosage Handbook, 3rd edn. Cleveland. LexiComp Inc, 1996-97; p 367.
51.
NIH Consensus Conference. Intravenous immune globulin: Prevention and treatment of disease.
JAMA 1990; 264: 3 I 89-3193.
52.
Nydegger UE. Safety and side effects of intravenous immunoglobulin therapy. Clin Exp Rheumatol 1996; 14: S53-S57.
53.
McCluskey DR, Boyd NA. Anaphylaxis with intravenous immunoglobulin. Lancet 1990; 336: 874.
|