Caffey disease or Infantile cortical hyperostosis, is a rare disorder of
unknown etiology, characterized by cortical hyperostosis with
inflammation of contiguous fascia and muscle [1]. It is self-limiting
and usually affects young infants. The diagnosis may be delayed as it
mimics a wide range of conditions like osteomyelitis, hypervitaminosis
A, bone tumor and child abuse. We present an infant with pseudoparalysis,
who was initially considered to have osteomyelitis of scapula, but was
later diagnosed to have Caffey disease.
 |
|
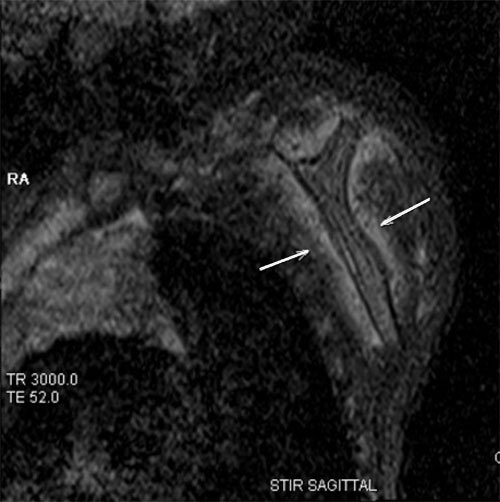
Fig. 1 MRI showing altered signal
intensity in the body of left scapula with periosteal reaction.
|
A 75-day-old boy with uneventful antenatal and
neonatal period, presented to us with complaints of paucity of movement
of left upper limb for one week. There was no history of fever,
intramuscular injection or trauma, lethargy or seizures. He was not on
any vitamin supplementation. On examination, he was irritable.
Neurological examination revealed paucity of movement of left upper
limb. Deep tendon reflexes were preserved. Detailed general examination
showed mild soft tissue swelling over the body of left scapula. Left
shoulder movement was painful. There was no other bony swelling or
tenderness. After consulting Orthopedician, chest X-ray and
magnetic resonance imaging (MRI) of left shoulder with upper limb was
done. MRI (Fig. 1) showed altered signal intensity in the
body of left scapula with periosteal reaction and adjacent soft tissue
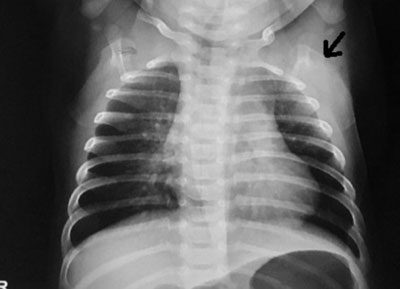
edema, features favoring osteomyelitis. Chest X-ray (Fig.
2) showed slightly thickened and sclerotic left scapula suggestive
of Caffey disease. Laboratory tests showed leukocytosis, anemia (Hb 8.4
g/dL), thrombocytosis, positive C-reactive protein (25.1 mg/L), and high
ESR (20 mm/hr). Blood culture was sterile. Infant was treated with
Ibuprofen. Left upper limb movement improved and infant is doing well on
follow-up.
 |
|
Fig.2 X-ray showing showing thickened
and sclerotic left scapula.
|
Though MRI was reported as osteomyelitis of scapula
in our infant, the absence of underlying risk factors for bone infection
made us suspect an alternative diagnosis. The presence of irritability,
soft tissue swelling and hyperostosis on X-ray helped us clinch
the diagnosis. Thrombocytosis has also been reported in caffey disease
[2]. Though Mandible is the most commonly involved bone, scapular
involvement presenting as Erb’s palsy has been earlier reported [3]. A
high index of clinical suspicion is required to diagnose Caffey disease
and avoid unnecessary investigations and intervention.
Acknowledgement: Dr S Muralinath for
radiology assistance.
References
1. Horton WA, Hecht JT. Disorders for which defects
are poorly understood or unknown. In: Nelson Textbook of
Pediatrics, 20th edn. Eds. Kliegman RM, Stanton BF, St. Gema JW, Schor
NF, Behrman RE. Philadelphia: WB Saunders Co, 2011. p.3379.
2. Krishnamurthy S, Srinivasan S. Severe
thrombocytosis as initial manifestation of Caffey disease in a 4 month
old infant. Pediatr Blood Cancer. 2012;59:345-6.
3. Holtzman D. Infantile cortical hyperostosis of scapula presenting
as Erb’s palsy. J Pediatr. 1972;81:785-8.


