|
|
|
Indian Pediatr 2017;54:147 -148 |
 |
Hemosuccus Pancreaticus
|
|
Sumathi Bavanandam and Nirmala Dheivamani
From Department of Pediatric Gastroenterology,
Institute of Child Health & Hospital for Children, Chennai, India.
Correspondence to: Dr Sumathi Bavanandam, Senior
Assistant Professor, Department of Pediatric Gastroenterology, Institute
of Child Health & Hospital for Children, Chennai 600 008, India.
Email:
drbsumathi@rediffmail.com
Received: April 04, 2016;
Initial review: May 19, 2016;
Accepted: December 22, 2016.
|
Background: Gastrointestinal bleeding in
children has diverse etiologies. Case characteristics: Two
children (age 3y and 7y) with recurrent gastrointestinal bleeding.
Computed tomography demonstrated features of chronic pancreatitis but no
vessel abnormality. Conventional angiography revealed bleeding from
gastroduodenal artery in both cases. Outcome: Coil
embolization of gastroduodenal vessels was performed, and there was no
recurrence of bleeding. Message: Hemosuccus pancreaticus
is to be considered in children with chronic pancreatitis presenting
with recurrent gastrointestinal bleeding and conventional angiography
with coil embolization is helpful.
Keywords: Angiography, Coil embolization, Hematemesis,
Pancreatitis.
|
|
R
ecurrent gastrointestinal bleeding is not
uncommon in children, and has diverse etiologies. Hemosuccus
Pancreaticus is defined as upper gastrointestinal bleed from papilla of
vater via pancreatic duct, and is a rare cause of life-threatening
gastrointestinal bleeding in children with either acute or chronic
pancreatitis [1,2]. Endoscopy during an attack is often rewarding and
conventional angiography has a therapeutic role.
Case Report
Case 1: A 3-year-old boy presented with recurrent
episodes of hematochezia and melena of varying severity, associated with
abdominal pain and progressive pallor of 6 months duration requiring
multiple blood transfusions. At one and half years of age, he was
conservatively treated for acute pancreatitis presenting with ascites.
Clinically he was anemic (Hb 7 g/dL), and undernourished (weight and
height below 3rd centile). Systemic examination was normal. Provisional
diagnosis of Hemosuccus pancreaticus was considered and investigated.
Liver function tests, serum amylase, lipase, and renal function tests
were normal. Upper endoscopy on three different occasions and
colonoscopy on two occasions were not contributory. CECT abdomen with
angiography showed features of chronic pancreatitis without any vessel
abnormality. An emergency gastroscopy was done during the episode of
hematochezia, which revealed active oozing of blood from ampulla
suggestive of Hemosuccus pancreaticus. Conventional angiography of
selective celiac axis/superior mesenteric artery (done elsewhere) showed
a leak in the gastroduodenal artery, and two coils (2mm × 2cm and 3mm ×
3cm) were deployed (Fig 1a). Child is asymtomatic on
follow up for more than a year.
 |
|
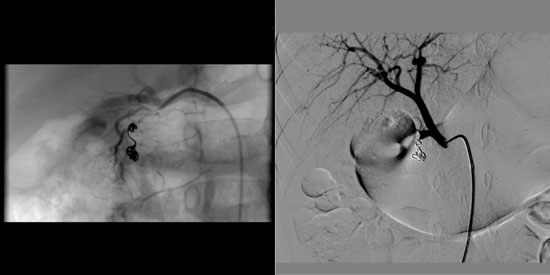
Fig. 1 Conventional angiography
showing coils deployed in the gastroduodenal branch (a) in first
case; and in the aberrant gastroduodenal branch (b) in the
second case.
|
Case 2: A-7-year-old boy presented with repeated
episodes of hematemesis and hematochezia associated with abdominal pain,
requiring multiple transfusions. His weight and height for age was below
-3SD. Clinical examination was unremarkable except for anemia.
Investigations showed Hb 7 g/dL with severe microcytic hypochromic
anemia. Liver functions tests, serum amylase, lipase and blood sugar
were normal. Ultrasound abdomen with Doppler showed pancreatic ductal
dilatation. CECT angiogram showed pancreatic duct dilatation with
calcification without any vessel abnormality. He was hemodynamically
stabilized. Upper gastrointestinal endoscopy on two occasions and
colonoscopy with terminal ileoscopy once done were normal. During the
hospital stay, following another bout of massive hematemesis, an
emergency endoscopy was done, which showed active bleeding from the
ampulla suggestive of Hemosuccus pancreaticus. Conventional angiogram
showed a clot in the gastroduodenal vessel with abnormal hepatic artery,
and coil embolization of the gastroduodenal artery with maestro wire was
done (Fig 1b). The patient is on follow-up for one year,
and is asymptomatic.
Discussion
Hemosuccus pancreaticus is an unusual cause of
potential life-threatening gastrointestinal bleeding occurring as a
complication of chronic or acute pancreatitis [1,2]. Apart from chronic
pancreatitis, other causes include tumours and vascular disorders [3].
Other terminologies are hemoductal pancreatitis, pseudohematobilia and
Wirsungorrhagia. It was first reported in 1931 by Lower and Farrell
[4,5]. Rupture of pseudoaneurysm caused by autodigestion of vessel wall
by pancreatic enzymes or cyst induced pressure necrosis results, in
bleeding. Splenic (60-65%), gastroduodenal (20-25%) and
pancreaticoduodenal (10-15%) arteries are commonly involved while
pseudoaneurysm of hepatic aretery (5-10%), and left gastric artery
(2-5%) is less common [6-8]. Both of our cases had a leak in the
gastroduodenal vessels. Clinical presentation includes anemia, recurrent
gastrointestinal bleed, abdominal pain and normal liver and pancreatic
enzymes. The diagnosis can be extremely difficult due to its rarity,
anatomical location and intermittent symptoms requiring, repeated upper
endoscopy, preferably during an acute episode of bleeding as observed in
our study. Doppler ultrasonography, CT-angiogram or MR-angiogram can
pick up pseudoaneurysm. Both of our children had leak from
gastroduodenal artery which was picked by conventional angiography, (the
gold standard test) that was followed by coil embolization. Arterial
embolization can arrest the bleeding in 67-100% of cases and should be
performed once patient is hemodynamically stabilized. In chronic
pancreatitis, selective arterial embolization may leave a chance of
recurrence due to remaining of diseased pancreas, adjacent to previously
injured vessel, but this can be minimized with the use of
super-selective angiocatheters in centers where technical expertise is
available. Surgical treatment is indicated in uncontrolled hemorrhage or
failed interventional procedures.
We conclude that hemosuccus pancreaticus can present
as recurrent gastrointestinal bleeding in children with chronic
pancreatitis. Conventional angiography with coil embolization are are
suitable methods for diagnosis and treatment, respectively.
Contributors: SB: Case work-up, management of
patient , drafting and editing the manuscript; ND: Case work-up,
management of patient.
Funding: None; Competing interest: None
stated.
References
1. Bivins BA, Schatello CR, Chuang VP, Brady P.
Hemosuccus pancreaticus (hemoductal pancreatitis): Gastrointestinal
hemorrhage due to rupture of a splenic artery aneurysm into the
pancreatic duct. Arch Surg. 1978;113:751-3.
2. Cahow CE, Gusberg RJ, Gottlieb LJ.
Gastrointestinal hemorrhage from pseudoaneurysms in pancreatic
pseudocysts. Am J Surg. 1983;145:534-41.
3. Han B, Song ZF, Sun B. Hemosuccus pancreaticus: a
rare cause of gastrointestinal bleeding. Hepatobiliary Pancreat Dis Int.
2012;11:479-88.
4. Koren M, Kinova S, Bedeova J, Javorka V, Kovacova
E, Kekenak L. Hemosuccus pancreaticus. Bratisl Lek Listy.
2008;109:37-41.
5. Sandblom P. Gastrointestinal hemorrhage through
the pancreatic duct. Ann Surg. 1970;171:61-6.
6. Stabile BE, Wilson SE, Debas HT. Reduced mortality
from bleeding pseudocysts and pseudoaneurysms caused by pancreatitis.
Arch Surg. 1983;118:45-51.
7. Heath D, Reid AW, Murray WR. Bleeding pseudocysts
and pseudoaneurysms in chronic pancreatitis. Br J Surg. 1992;79:281.
8. Negi SS, Sachdev AK, Bhojwani R, Singh S, Kumar N.
Experience of surgical management of pseudoaneurysms of branches of the
coeliac axis in a North Indian hospital. Trop Gastroenterol.
2002;23:97-100.
|
|
|
 |
|
