Headache is a common problem in
children and causes significant disability [1]. Robust diagnostic
criteria are essential due to its high prevalence and the absence of any
diagnostic investigations. The International Classification of Headache
Disorders, 3
rdedition
(ICHD-3) has been released by the ‘International Headache Society’ in
May 2013 [2]. As this version is based on a large body of research on
headache, in contrast to previous editions that were mostly based on
opinion of experts, it is being considered as a major step forward in
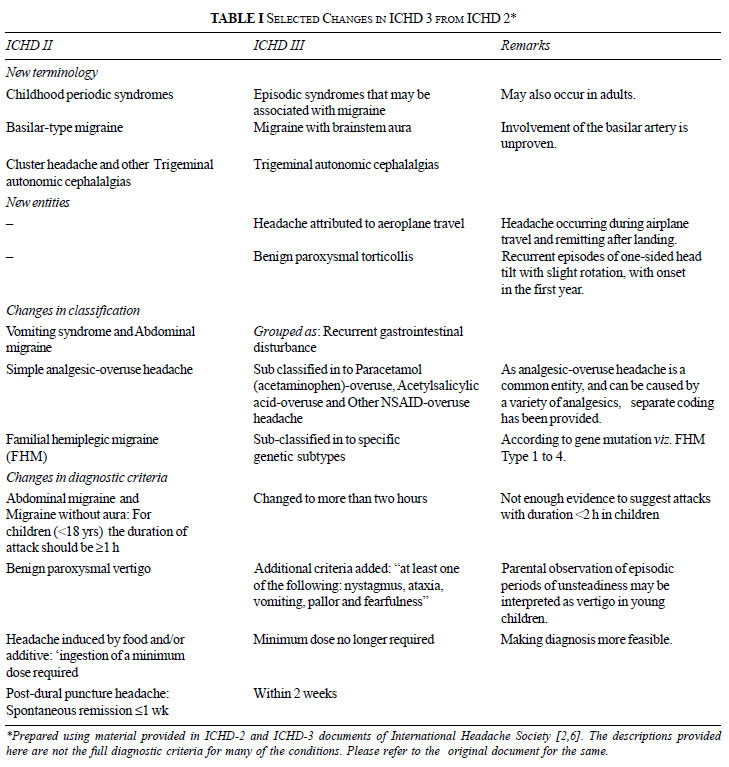
the diagnosis and management of headache [3]. We herein present the
salient features of the new classification, which are likely to be of
interest to the pediatricians. The important ones include change in some
terminologies, addition of new categories and changes in diagnostic
criteria, and have been summarized in Table I.
 |
| |
The most important change has been in the diagnosis
of ‘Secondary’ headaches, which will be of interest to those in
developing countries because of the high numbers of such headaches
[4,5]. When a new headache occurs in close temporal relation to another
disorder that is known to cause headache (or fulfills other criteria for
causation by that disorder), it is coded as Secondary headache,
attributed to the causative disorder even if the headache has the
characteristics of a Primary headache (migraine, tension-type headache,
etc.) [3]. ICHD-2 required ‘remission or substantial improvement of the
underlying causative disorder’ before the diagnosis of Secondary
headache could be made [6]. The new diagnostic criteria can thus be
applied at presentation, or as soon after as the underlying disorder is
confirmed. In acute conditions, a close temporal relation between onset
of headache and onset of the presumed causative disorder is often
sufficient to establish causation, whereas less acute conditions usually
require more evidence of causation.
The other important change is in the category
‘Childhood periodic syndromes that are commonly precursors of migraine’
(benign paroxysmal vertigo of childhood, cyclical vomiting and abdominal
migraine) [6] that have now been renamed as ‘Episodic syndromes that may
be associated with migraine’, and have an additional condition Benign
paroxysmal torticollis. Cyclical vomiting and Abdominal migraine have
been clubbed together as ‘Recurrent gastrointestinal disturbance’ [2].
The changes in ICHD-3 have been presented here in an
abridged form. Those interested in a more detailed study of these
guidelines may see the full document or visit the International Headache
Society website for further information (www.ihs-headache.org).
Contributors: Both authors were involved in
literature search, the drafting the manuscript and its approval.
Funding: None; Competing interests: None
stated.
References
1. Mishra D, Sharma A, Juneja M, Singh K.
Recurrent headache in pediatric outpatients at a public hospital in
Delhi. Indian Pediatr. 2013;50:775-9.
2. Headache Classification Committee of the
International Headache Society. The international classification of
headache disorders, 3rd edition. Cephalalgia. 2013;33: 629-808.
3. Olesen J. ICHD-3 beta is published. Use it
immediately. Cephalalgia. 33:627-8.
4. Mishra D. Cysticercosis headache: an important
differential of childhood headache disorder in endemic countries.
Headache. 2007;47:301-2.
5. Kumar V, Gulati A, Mehra B. Cysticercosis of
the temporalis muscle causing temporal headache in a pregnant woman.
Int J Gynaecol Obstet. 2011;114:79.
6. Headache Classification Committee of the International Headache
Society. The International classification of headache disorders, 2nd
edition. Cephalalgia 2004;24: 1-160.


