|
|
|
Indian Pediatr 2013;50: 237-239
|
 |
Thalidomide for Systemic Onset Juvenile
Idiopathic Arthritis
|
|
K Sathe and RP Khubchandani
From the Department of Pediatrics, Jaslok Hospital &
Research Centre, Mumbai, India
Correspondence to: Dr Raju Khubchandani, 31
Kailas Darshan, Nana Chowk, Kennedy Bridge,
Mumbai 400 007, MS, India.
Email:
[email protected]
Received: July 07, 2012;
Initial review: August 06, 2012;
Accepted: August 23, 2012.
|
Systemic onset juvenile idiopathic arthritis (SOJIA) is the most common
autoimmune auto inflammatory disease in childhood. A sizeable number of
these patients run a recalcitrant disease course, resistant to the
conventional line of management, ultimately resulting in permanent
disability from joint destruction, local growth deformities or
iatrogenic side effects. The new biological agents although very
effective, are beyond the affordability of most in our country.
Thalidomide, a cheaper option has been shown to be very effective in the
disease control of patients with SOJIA. We report three Indian children
with a chronic refractory course of SOJIA, all of whom had failed
conventional line of treatment but improved with thalidomide.
Keywords: Thalidomide, Juvenile idiopathic arthritis.
|
|
More than 40% of children with juvenile
idiopathic arthritis present with systemic onset juvenile
idiopathic arthritis (SOJIA) in India [1], in contrast with 10%
in the Western population. The disease is characterized by
dominant systemic features associated with or without arthritis
and usually runs a polycyclic course with multiple exacerbations
and remissions with almost 50% patients eventually recovering
completely, while the rest run a progressive downhill course of
disabling arthritis [2]. The conventional treatment options can
completely control the disease in only about 60% cases [3]. The
realization of the role of the proinflammatory cytokines in the
pathogenesis of SOJIA has led to introduction of newer
biological agents for management. However, their prohibitive
cost remains the greatest obstacle in their use in the
economically weaker section.
Thalidomide, once discarded as a potent
teratogen, has been reported effective in the management of
SOJIA on account of its immunomodulatory properties [2,4].We
share our experience in managing three patients with refractory
course of SOJIA.
Case Report
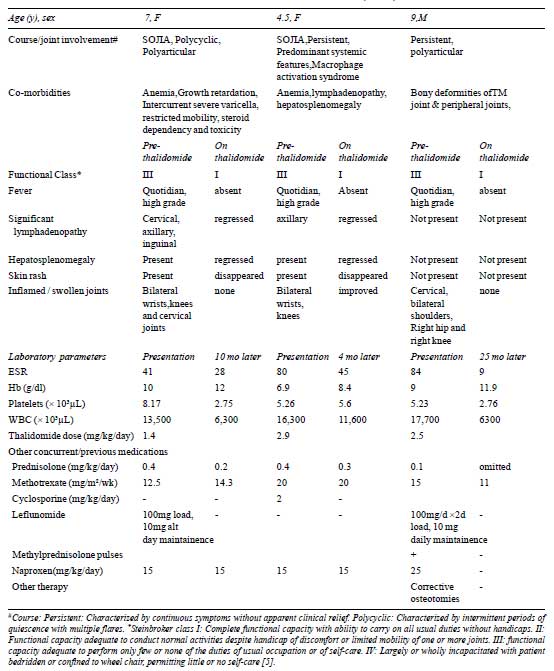
Details of the children are presented in
Table I. Case 1 improved in the form of mobility and
physical well being, weight gain, decrease in mean joint count
and normalization of acute phase reactants.At 10 months post
thalidomide follow up she was off steroids and there was
functional improvement from Steinbroker class 3 to class 1
without any side effects of therapy. Case 2 improved with
remission of fever, improved physical mobility, decrease in mean
joint count and normalization of acute phase reactants. At 4
months post thalidomide follow up the steroids were completely
stopped with functional improvement from class 3 to class 1
without any adverse effects of therapy. Case 3, over a
period of follow up of 25 months after starting thalidomide,
showed improved mobility with minimal aids, decrease in the mean
joint count and functional improvement from Steinbroker Class 3
to 1 without any adverse effects of therapy.
TABLE I Three Children with Systemic Onset Juvenile Idiopathic Arthritis (SOJIA) Managed With Thalidomide
Discussion
All the three children had failed multiple
conventional drugs before being started on Thalidomide. They
were all offered biological therapy but refused after being
explained the cost of therapy. The background history of
thalidomide was explained to them and one adolescent girl
refused the drug. It was started after due informed consent at a
dose of 2-3 mg/kg/day in a nightly dose to combat its sedative
side-effects. They were all steroid-dependent with its attendant
short and long term side effects in the form of osteoporosis,
infections and growth retardation. They all had significant
improvement after beginning thalidomide therapy. There was
normalization of the acute phase reactants (hemoglobin, total
counts, platelets and ESR), decrease in the mean joint count and
improvement in physical wellbeing and growth. There was
functional improvement from Steinbroker class III to class I [5]
and could be successfully weaned off steroids. Thus they all
achieved inactive disease stage as per Wallace criteria [6].
Thalidomide is a unique immunomodulator agent
with an anti-angiogenesis effect in addition to inhibition of
TNF- a.
TNF-a
is a potent pro-inflammatory cytokine, over-production of which
has been implicated in mouse models of inflammatory arthritis
and also in plasma and synovial fluid in patients with active
arthritis including children with JIA. Thalidomide is also
thought to suppress other proinflamatory cytokines including
IL-6 [2,7], to down regulate adhesion molecules as well as to
inhibit leukocyte chemotaxis and decrease the CD4/CD8 ratio
[2,7]. Evidence concerning the use of thalidomide in SOJIA is
limited [4]. In the largest of these studies, Lehman, et al.
[4] and colleagues have reported the use of thalidomide (2 to 5
mg/kg/day) in 13 children with severe, refractory SOJIA. Six
children were able to discontinue chronic steroids, thus
highlighting its steroid sparing effect.
Thalidomide being a potent teratogen,
birth-control is necessary for both males and females and
extreme caution would be necessary when our patients achieve
adolescent or child-bearing age. Another major though rare
adverse effect is permanent peripheral neuropathy with long term
use, for which, regular monitoring including physical
(neurological) examination and nerve conduction velocity studies
need to be performed [7]. We routinely enquire about the
occurrence of tingling, numbness, paraesthesiae and perform a
detailed neurological exam in all the three patients on every
follow-up visit. So far we have not had reason to suspect
peripheral neuropathy in any of our children.
Other side effects include sedation,
somnolence, myalgia, constipation, neutropenia and anaphylaxis.
The tolerability is generally found to be better with single
night time administration. It is also highly economical,
(approximate Rs 40/- per tablet of 50 mg the daily dose for a
15-25 kg child), which is in sharp contrast to the other reserve
drugs available for this disease.
We advocate careful closely supervised use of
thalidomide in consenting refractory cases of SOJIA where
biologicals are unaffordable. Larger studies in our country on
this ‘poor man’s biological’ are in order.
Contributors: Both authors were
involved in the acquisition, analysis and interpretation of
data, drafting the manuscript, critical revision of the
manuscript and final approval of the version to be published.
Funding: None; Competing interests:
None stated.
References
1. Sarma PK, Misra R, Aggarwal A. Physical
disability, articular, and extra-articular damage in patients
with juvenile idiopathic arthritis. Clin Rheumatol.
2008;27:1261-5.
2. Hayward K, Wallace CA. Recent developments
in anti-rheumatic drugs in pediatrics: treatment of juvenile
idiopathic arthritis. Arthritis Res Ther. 2009;11:216.
3. Gianini EH, Brewer EJ, Kuzmina N, Shaikov
A, Maximov A, Vorontsov I, et al. Methotrexate in
resistant juvenile rheumatoid arthritis. N Engl J Med.
1992;326:1043-9.
4. Lehman TJ, Striegel KH, Onel KB.
Thalidomide therapy for recalcitrant systemic onset juvenile
rheumatoid arthritis. J Pediatr. 2002;140:1:125-7.
5. Hochberg MC, Chang RW, Dwosh I, Lindsay S,
Pincus T, Wolfe F. The American College of Rheumatology 1991
Revised Criteria for the Classification of Global Functional
Status in Rheumatoid Arthritis. Arthritis Rheumat.
1992;35:5:498-502.
6. Ravelli A, Martini A. Remission in
juvenile idiopathic arthritis. Clin Exp Rheumatol. 2006;43:S
105- 10.
7. Re-emergence of Thalidomide. Indian J
Pharmacol. 2003;35:204-12.
|
|
|
 |
|