|
We report a two years old girl who was born preterm
at 36 weeks with a birth weight of 2.6 kg to a primi mother by emergency
cesarean section due to uncontrolled hypertension. Mother’s age was 24
years and she was hypothyroid, hypertensive and had Type 2 diabetes
mellitus. She was on thyroxine, nifedipine and oral hypoglycemics, which
was changed to insulin during pregnancy.
Baby was hypotonic and lethargic. TSH was >100mlU/L.
She was started on oral thyroxine and discharged on 7 th
day of life. At 6 months, baby presented with fast breathing. Heart rate
was 180/min, respiratory rate was 68/min and the baby looked flushed.
Thyroxin induced hyperthyroidism was suspected. Blood pressure recording
in right upper arm was 140/100 mmHg. Her thyroid profile was within
normal limits.
Child was put on propranolol and was investigated for
secondary causes of hypertension. Renal function test, plasma
adrenaline, noradrenaline; urine 24 hours metanephrine, 24 hours VMA;
serum cortisol, aldosterone, and renin were within normal limits. CT
abdomen showed normal sized kidneys and normal appearing liver and
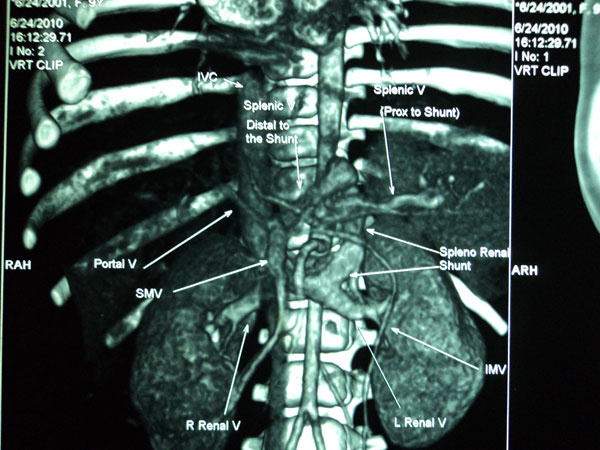
spleen. Echocardiography was with in normal limits. CT renal angiography
showed single renal artery on both sides with no coarctation or
aneurysm, single renal veins on both sides, abnormal large spenorenal
shunt between splenic vein and left renal vein, left renal vein dilated
measuring 1.1 cm, shunt measured 0.6 cm, portal vein narrowed to 0.2 cm
(Fig.1).
 |
|
Fig.1 CT renal angiography showing
large splenorenal shunt.
|
Presently the child is on propranolol 5 mg twice a
day, and L-thyroxine 50 µg daily. Her growth and milestones are with in
normal limits. Her BP and thyroid status is with in range.
Our dilemma was whether hypertension is due to the
splenorenal shunt and the future management of this shunt. Pulmonary
hypertension has been reported in cases with congenital porto-systemic
venous shunt but we could not get any literature reporting systemic
hypertension in this condition. Extremely hypoplastic kidneys have been
reported in an aborted fetus with congenital splenorenal venous shunt.
But ultrasonography shows bilateral normal size kidneys in this child.
It is reported that patients with congenital
splenorenal shunt may be asymptomatic in the initial years but develop
portosystemic encephalopathy at later stage. Hepatic cirrhosis has also
been reported. We are following her with serial ammonia levels which is
with in normal limits. CT guided liver biopsy shows normal histology.
References
1. Ohno T, Muneuchi J, Ihara K, Yuge T, Kanaya Y,
Yamaki S, et al. Pulmonary hypertension in patients with
congenital portosystemic venous shunt: a previously unrecognized
association. Pediatrics. 2008;121:e892-9.
2. Ji EK, Yoo SJ, Kim JH, Cho KS. Congenital
splenorenal venous shunt detected by prenatal ultrasonography. J
Ultrasound Med. 1999;18:437-9.
3. Ishii Y, Inagaki Y, Hirai K, Aoki T. Hepatic
encephalopathy caused by congenital extrahepatic portosystemic venous
shunt. J Hepatobiliary Pancreat Surg. 2000;7:524-8.
4. Yamagami T, Nakamura T, Iida S, Kato T, Tanaka O,
Matsushima S, et al. Hepatic encephalopathy secondary to
intrahepatic portosystemic venous shunt: balloon-occluded retrograde
transvenous embolization with n-butyl cyanoacrylate and microcoils.
Cardiovasc Intervent Radiol. 2002;25:219-21.
5. Ishii Y, Inagaki Y, Hirai K, Aoki T. Hepatic encephalopathy caused
by congenital extrahepatic portosystemic venous shunt. J Hepatobiliary
Pancreat Surg. 2000;7:524-8.
|


