|
|
|
Indian Pediatr 2011;48: 143-145 |
 |
Cyclical Vomiting Syndrome with Bilateral
Epileptiform Discharges |
|
Saurabh S Chopra, Shilpa D Kulkarni, Anaita U Hegde and Krishnakumar N
Shah
From MP Shah Medical College, Jamnagar; and BJ Wadia
Hospital for Children, Mumbai, India.
Correspondence to: Saurabh S Chopra, B-8 Mahavir Appt,
Opp Pratap Villas, Jamnagar 361 008, India.
Email:
saurabh_dr1@rediffmail.com
Received: May 11, 2009;
Initial review: April 13, 2009;
Accepted: September 15, 2009.
|
Cyclical vomiting syndrome is a paroxysmal, condition characterized by
recurrent severe episodes of vomiting lasting for hours to days, with
variable intervals of normal health in between with no apparent cause of
the vomiting. We hereby report a 10yr old girl with cyclical vomiting
syndrome with multiple, bisynchronous occipitally predominant, bilateral
epileptiform discharges representing a diagnostic confusion.
Key words: Cyclical vomiting, Occipital spike, Panayiotopoulos
syndrome.
|
|
We report a girl with cyclical vomiting
syndrome with multiple, occipitally predominant, bilateral epileptiform
discharges represen-ting a diagnostic dilemma. Although there are multiple
reports of epileptiform discharges with migraine, we believe that cyclical
vomiting syndrome with epiletiform discharges represents an unusual
clinical situation.
Case Report
A 10-year old girl born of a non-consanguineous
marriage presented with complaints first noticed since 5 years of age. She
had paroxysmal stereotyped episodes starting with feeling of uneasiness,
nausea and abdominal pain, followed by repeated episodes of non-bilious,
non-projectile vomiting about 40-50/day. The episodes usually continued
for few hours to 3-4 days (ranging from only transient feeling of nausea
relieved by anti-emetics to vomiting episodes lasting for 10-15 days). She
had multiple episodes of dehydration due to vomiting warranting parenteral
fluid resuscitations. Occasional mild non-specific headache occurred after
prolonged episodes of vomiting. These paroxysms were precipitated by
psychological stressors related to academics, extra curricular activities
etc. and were partially or completely relieved by sleep. Paroxysms
averaged around 3-4/year.
There was no history of visual hallucinations or of any
seizure episodes. The child was otherwise totally normal in between
episodes, well nourished, above average in school and good at extra
curricular activities.
 |
|
 |
|
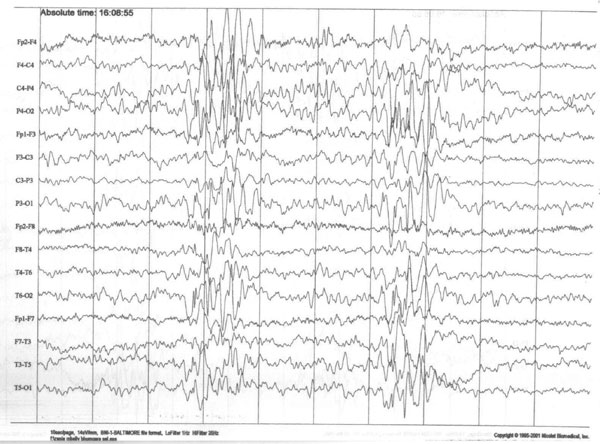
Fig. 1 Sleep EEG of the patient showed
multiple brief bi-synchronous spike and wave discharges with
occipital predominance. |
Before being referred to us, the child was extensively
investigated. Hemogram, electrolyte, liver and kidney functions,
ultrasonography of the abdomen, upper GI endoscopy, Barium-studies and
work-up for H. pylori all were normal. At our center Video-EEG for
4 hour was performed and two minor vomiting episodes were captured. Inter-ictal
EEG showed brief bi-synchronous spike and wave discharges with occipital
predominance and anterior spread, mainly during sleep. EEG did not show
any ictal correlate during vomiting except for bisynchronous posterior
spike and wave complexes lasting briefly on one occasion, not starting and
ending with the event. MRI brain was normal. The patient was started on
topiramate and counseling was provided for better management of stress and
regular routine daily activities. Significant improvement in symptoms was
noted over the next 15 months, with no episodes of nausea or vomiting
during the last 12 months.
Discussion
Cyclical vomiting syndrome (CVS) is a paroxysmal
condition characterized by recurrent severe episodes of vomiting lasting
for hours to days, with variable intervals of normal health in between and
no apparent cause of the vomiting. CVS is a condition of unknown etiology
and pathogenesis, however, support exists for it to be a migraine
equivalent [1,2]. EEG changes documented include abnormal delta waves that
disappear when the patient is asymptomatic [2]. Another report documents
brief epileptoform discharges in form of sharp wave complexes that were
seen during hyperventilation and once during the episode itself but not
starting and ending with the event [3].
Before diagnosing CVS other possible etiologies of
episodic vomiting need to be considered. In our patient gastrointestinal
causes like malrotations, H.pylori infection, renal and hepatic
causes were ruled out. The symptom complex also did not suggest inborn
errors of metabolism, urea cycle disorders, mitochondrial diseases or
porphyria. A normal neuroimaging and absence of visual symptoms made
symptomatic occipital epilepsyand Gastaut’s epilepsy unlikely. The
prominence of vomiting as compared to abdominal pain or headache in our
patient prompted us to classify her as CVS instead of abdominal migraine
[1]. Thus our patient
fulfilled all essential clinical criteria for CVS [1]. However, paroxysms
of vomiting with epileptiform discharges predominantly in the occipital
region made Panayiotopoulos syndrome (PS) a definite possibility [4,5].
Clinically PS seemed less likely because the duration
of autonomic status is usually not more than seven hours, but prolonged
duration of symptoms in our patient lasting days is well known in CVS
[1,6]. Other points against PS were the absence of any other ictal
manifestations and complete preservation of orientation, which are unusual
in PS (10% and 6% respectively). PS has an active seizure period of 1-2
years only [5].
Video-EEG captured two vomiting episodes, one of which
revealed bisynchronous posterior spike and wave complexes lasting briefly
not starting or ending with the vomiting episode. Thus they could not be
considered to be ictal correlates. Few reports of ictal-EEG in PS report
rhythmic theta or delta activity usually intermixed with small spikes
[4,5]. The reports that such EEG changes could occur during developmental
stages without clinical manifestations raised the possibility that they
were just incidental findings [6]. Family history of headache and vomiting
was initially considered non-specific but could point towards a migraine
disorder.
Studies done to differentiate the electroclinical
features of migraine versus epilepsy in patients with occipital
epileptiform EEG abnormalities have concluded that bilateral abnormalities
correlate with migraine whereas unilateral abnormalities correlate with
epilepsy. Although no such studies could be found for CVS versus epilepsy,
CVS being a migrainous disorder- extrapolating the finding to our case,
indicate that since our patient had bilateral EEG abnormalities she is
more likely to have a migrainous disorder [7].
Thus, in spite of the apparent diagnostic confusion, it
was decided that the patient fitted more into CVS. Instead of the
conventional drugs like cyproheptadine and flunarizine, citing a previous
report with similar findings, Topiramate having both anti-migrainous and
anti-epileptic action was started with good results [3]. In concordance
with the case reported by Olmez, et al. [3] our case demonstrates
that EEG/video-EEG should be considered in patients of cyclincal vomiting
syndrome. Topiramate may be considered in managing the subset with
abnormal epileptiform discharges.
Contributors: All authors contributed to diagnosis
and management of the case and contributed to drafting the paper.
Funding: None.
Competing interests: None stated.
References
1. Marcus S, Sundaram S, BUK Li. Cyclic vomiting
syndrome. Available from http://www.emedicine. com/ped/TOPIC2910.HTM.
Accessed September 12, 2006.
2. Jernigan SA, Ware LM. Reversible quantitative EEG
changes in a case of cyclic vomiting: evidence for migraine equivalent.
Dev Med Child Neurol. 1991; 33:80-5.
3. Olmez A, Köse G, Turanli G. Cyclic vomiting with
generalized epileptiform discharges responsive to topiramate therapy.
Pediatr Neurol. 2006;35:348-51.
4. Covanis A, Ferrie CD, Koutroumanidis M, Oguni H,
Panayiotopoulos CP. Panayiotopoulos syndrome and Gastaut type idiopathic
childhood occipital epilepsy. In: Roger J, Bureau M, Dravet CH,
Genton P, Tassinari CA, Wolf P, editors. Epileptic Syndromes in Infancy,
Childhood and Adolescence. 4th ed. Montrouge, France: John Libbey Eurotext
Ltd; 2005. p. 227-53.
5. Panayiotopoulos CP. Early onset benign childhood
seizures with occipital spikes (Panayiotopoulos syndrome). Available from:
URL: http://www.ilae-epilepsy.org/Visitors/Centre/ctf/pana_synd.cfm.
Accessed on September 29, 2007.
6. Talwar D, Rask CA, Torres F. Clinical manifestations
in children with occipital spike-wave paroxysms. Epilepsia. 1992;33:
667-74.
7. Brinciotti M, Di Sabato ML, Matricardi M, Guidetti
V. Electroclinical features in children and adolescents with epilepsy
and/or migraine, and occipital epileptiform EEG abnormalities. Clin
Electroencephalogr. 2000; 31:76-82.
|
|
|
 |
|
