|
|
Short Communications Indian Pediatrics 2008; 45: 144-147 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Evaluation of Lactate Dehydrogenase, Creatine Kinase and Hepatic Enzymes for the Retrospective Diagnosis of Perinatal Asphyxia Among Sick Neonates |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sanath Reddy, Sourabh Dutta, and Anil Narang From the Newborn Unit, Department of Pediatrics,
Postgraduate Institute of Medical Education and Correspondence to: Dr Sourabh Dutta, Additional
Professor, Newborn Unit, Department of Pediatrics, Manuscript received: February 2, 2007; Initial review
completed: May 15, 2007;
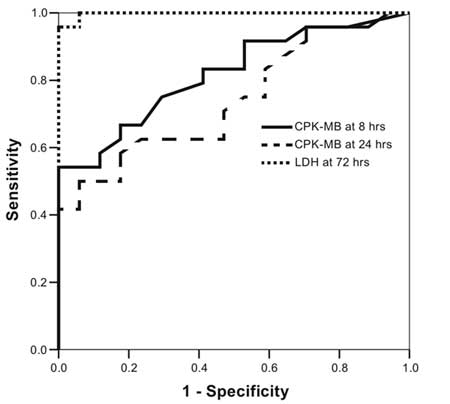
Introduction In India, 8.4% of inborn babies have a 1 minute Apgar score less than 7 and 1.4% suffer from hypoxic ischemic encephalopathy (HIE)(1). Only a third of deliveries in India are institutional(2) and many asphyxiated babies are brought late to hospitals. The signs of asphyxial injury are non-specific and overlap with other illnesses. In the absence of perinatal records, it is difficult to retrospectively diagnose perinatal asphyxia. We conducted this study to ascertain whether common enzyme assays in neonates with non-specific sickness can distinguish an asphyxial from a non-asphyxial etiology. Methods This prospective, matched cohort study was conducted on babies admitted to a level III neonatal unit. Cases and Controls comprised of asphyxiated and non-asphyxiated babies, respectively. Study subjects included 45 neonates (convenience sample) delivered at ³33 wks of gestation with birth wt ³1250 g; the delivery was attended by a pediatrician; and they became symptomatic within 6 hours of birth with at least 1 non-specific sign of sickness–tachypnea, chest retractions, grunt, lethargy, poor feeding, hypotonia, irritability, central cyanosis, cardiac gallop rhythm, cardiac murmur, shock and abdominal distension. Gestation was assessed from last menstrual period, early fetal ultrasound and New Ballard score. Birth weight was recorded electronically with least count of 1 g. Babies with major malformations, those born to mothers who had received pethidine, or magnesium sulphate within 4 h prior to delivery or who had obvious signs of HIE were excluded. Subjects were enrolled after written, informed consent from a parent. The study was approved by the Institute Ethics Committee. Cases were subjects with 1 minute Apgar score of <7 and fetal bradycardia, meconium stained liquor or cord pH <7; and without any other independent cause for the clinical signs. Controls were unasphyxiated neonates with normal fetal heart rate patterns, clear liquor, cord pH >7.20 and 1 min Apgar score ³7. Maternal and neonatal details were recorded. In all subjects, serum creatine kinase muscle-brain fraction (CK-MB) was performed at 6±1 h and 24±2 h; and serum lactate dehydrogenase (LDH), serum glutamic oxaloacetic transaminase (SGOT) and serum glutamic pyruvate transaminase (SGPT) at 72±2 h. Laboratory technicians were masked to the identity of the subjects. Serum CK-MB was analyzed by immunoassay on 1 mL clotted blood(3). A value above 92.6 U/L at 8 hours and above 60 U/L at 24 hours was abnormal(4). Serum LDH was analyzed by the liquiUV test on 1 mL clotted blood(5). A value above 580 U/L was abnormal(4). SGOT and SGPT were analyzed by standard methods on 1 mL clotted blood. Values of SGOT above 140 U/L and SGPT above 50 U/L were abnormal(4). Baseline characteristics and clinical and laboratory data were described by descriptive statistics. Cases and Controls were compared by Mann Whitney U test for skewed numerical variables and Fisher’s exact test for categorical variables. Sensitivity, specificity and predictive values of the tests were calculated. ROC curves were generated and the areas under the curve were compared to determine the most appropriate laboratory parameter. Results Cases (n=25) and Controls (n=20) had similar rates of prematurity (52% vs. 70%), male sex (64% vs. 90%), primi gravida mothers (52% vs. 35%), incidence of prolonged labour (0 vs. 7%) and prolonged rupture of membranes (18% vs. 36%). Significantly more Cases, as compared to Controls, were delivered by emergency cesarean section [14 (58%) vs. 3 (15%); P=0.003]. Ninety-two percent Cases had fetal bradycardia, 8% were born through meconium stained liquor and 48% cases had a cord pH <7. Eighty-four percent Cases required ventilation by bag-and-mask, 20% intubation and 8% chest compression. Apgar score was <7 in 48% and 10% subjects at 5 and 10 minutes of age, respectively. Among the symptoms, "hypotonia" was commoner in the Cases than Controls [17 (68%) vs. 0; P<0.001] and vice versa for "poor feeding" [12 (48%) vs. 16 (80%); P=0.02]. There was a trend for "shock" to be more common among Cases than Controls [4 (16%) vs. 0; P=0.06]. Other symptoms were not significantly different between both groups. No subject had clinical features of Stage III HIE by Sarnat and Sarnat scoring or Grade III by Levene’s classification(6,7). Comparative values of all enzymes in the 2 groups is shown in Table I. The sensitivity, specificity and predictive values of CK-MB and LDH are depicted in Table II. Receiver operator characteristics (ROC) curves were generated for CK-MB at 8 hours, 24 hours and LDH at 72 hours (Fig. 1). The area under curve for LDH was 0.998 [95% C.I. 0.99, 1.0 (P<0.001)]. The area under curve for CK-MB at 8 hrs was 0.82 [95% C.I. 0.69, 0.94 (P=0.01)]. The area under curve for CK-MB at 24 hrs was 0.74 [95% C.I. 0.59, 0.89 (P=0.009)]. TABLE I Comparison of Levels of Enzymes Between Cases and Controls
CK-MB: Creatine kinase muscle brain fraction; LDH: Lactate dehydrogenase; SGOT: Serum glutamic oxaloacetic transaminase; SGPT : Serum glutamic pyruvate transaminase TABLE II Sensitivity, Specificity and Predictive Values of Enzymes
CK-MB: Creatine kinase muscle brain fraction; LDH: lactate dehydrogenase Discussion This study showed that LDH at 72 hours of life was the most accurate test for discriminating asphyxia from other illnesses among neonates who presented with non-specific signs of illness. The strength of our design was that it resembled sick patients in real-life clinical scenarios. None of the subjects had severe grades of HIE, whose diagnosis is generally obvious. Seventeen cases had hypotonia, of which 13 also had lethargy, but there were no other features of encephalopathy. This design was unlike many previous studies that had either compared asphyxiated neonates with healthy controls; or had evaluated asphyxiated neonates, irrespective of whether they became symptomatic; or had limited their case selection only to those who had HIE.
Jedeiken(8) described that the normal levels of all iso-enzymes of CK in newborns peaked at 5-33 hours postnatally. In a study by Primhak, et al.(9), the CK-MB in both normal (n=43) and asphyxiated (n=20) neonates, peaked at 8 hours and fell by 72 hours. Absolute and percen CK-MB levels were higher in asphyxiated babies. Sanchez-Nava, et al.(10) showed that SGOT, SGPT and LDH were raised among asphyxiated babies. The levels of the above enzymes are also raised in other sick infants, but the magnitude of elevation is higher in asphyxiated neonates. Barberi, et al.(11) reported that CK, CK-MB, CK-MB/CK ratio and LDH were all increased in an asphyxiated group, while in a group with respiratory distress, only CK-MB and the CK-MB/CK ratio were abnormal. Lackmann, et al.(12) found that newborn infants with asphyxia have significantly higher values of SGOT, LDH and hydroxybutyrate compared to neonates with only RDS, and presence of RDS among asphyxiated neonates did not alter the enzyme levels. The results of the present study would be of utility to pediatricians in referral hospitals, who receive sick neonates, whose birth details are not well recorded. LDH could be used at 3 days of age to diagnose asphyxia retrospectively in such cases. It is not possible to draw any conclusions regarding the utility of LDH before or after 72 hours. A limitation was that we did not exclude subjects with hemolysis or hepatitis who could have had an increase in LDH due to reasons other than asphyxia. Acknowledgments We gratefully acknowledge the help provided by Dr Rajendra Prasad and his group in the Pediatric Biochemistry laboratory in analyzing lactate dehydrogenase. Contributors: SR collected the data and samples, SD analyzed the results and wrote the manuscript, AN provided the concept and supervised the manuscript. Funding: None. Competing interests: None stated.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()