|
|
Case Reports Indian Pediatrics 2007;44:144-147 |
||||
|
PHACES Syndrome with Congenital Hypothyroidism |
||||
|
Apurba Ghosh
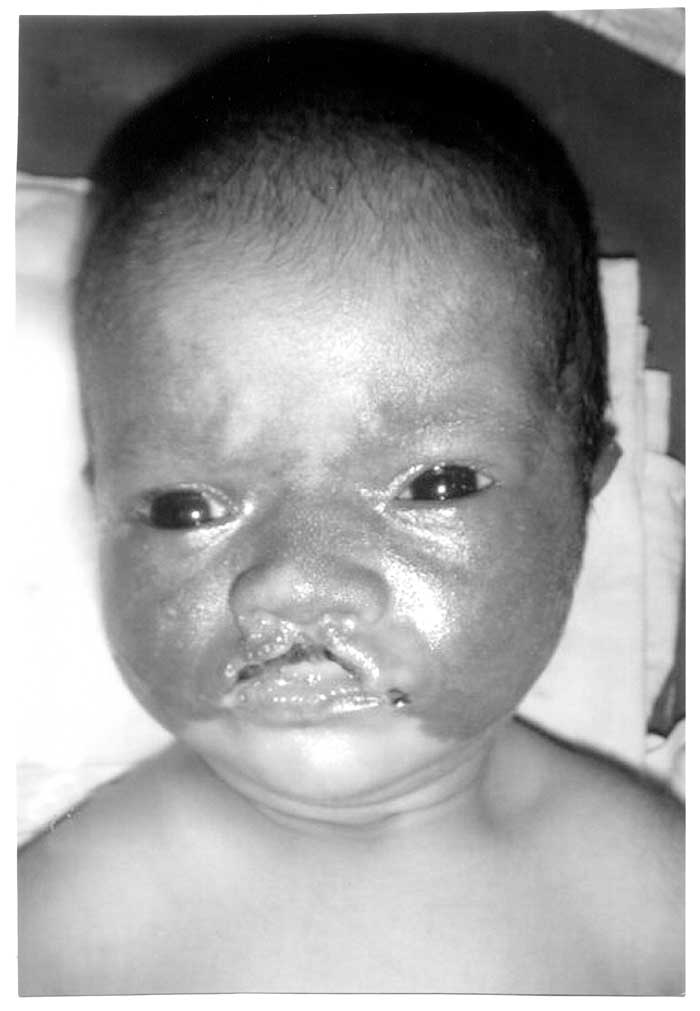
Abstract: Key words: Dandy Walker cyst, Hemangioma, PHACES. Hemangiomas are the most common tumor of infancy, occurring in up to 10% of all infants(1). In majority of cases, they are not associated with other abnormalities. Occasionally, they may indicate the presence of systemic malformations. The association of cerebrovascular and facial arterial anomalies and the hemangiomas was first noticed by Pascual-Castroviejo in 1978(2). Later Reese, et al.(3) in 1993 described the association of facial hemangiomas with Dandy Walker and other posterior fossa malformations(3). The acronym PHACE was proposed by Frieden, et al. in 1996(4). Case Report A 20-day-old female neonate, delivered at term by LSCS and born out of non-consanguineous marriage presented reddish skin lesions involving the face and the scalp at 2 days of life, associated with progressive erosion of the upper lips since 5 days of life. She also had two episodes of tonic convulsion that subsided spontaneously. The baby was on breast feed since birth but was having feeding difficulties few days prior to admission. Ultrasound scan done at 30 weeks of gestation had revealed Dandy Walker cyst. On examination the weight of the baby was 2.65 kg, length 52 cm and head circumference 34 cm. The physical examination was normal except for a large flat hemangioma covering almost the entire face extending onto the scalp, including the mandibular region. Upper lip was eroded with ulcerative changes (Fig.1) Hemangioma was absent at other sites including the subglottic region. Sternal pits were noted on careful palpation of the chest. Neurologic examination was normal. The examination of other systems was unremarkable. Hematological investigations were normal. Liver function tests, serum urea, creatinine and electrolytes were normal. Chest radiograph and ECG were normal. MRI Brain showed the presence of Dandy Walker cyst (Fig.2). Echocardiography including Doppler study of subclavian arteries was normal. Ophthalmologic examination was normal. Thyroid profile was consistent with the diagnosis of congenital hypothyroidism (T4: 3.2 mcg/100 mL; TSH: 48.4 micro IU/mL). The parents were advised a thyroid scan but they could not afford it.
The baby was put on oral phenobarbitone. Further episodes of convulsions were not noted during the course of hospital stay. Appropriate management of hypothyroidism was started using oral thyroxine. The baby was allowed expressed breast milk with katori and spoon. We intend following the baby on a regular basis. The parents were counseled regarding the prognosis and complications of the disease. Discussion PHACES syndrome is a phakomatosis which is easily confused with Sturge Weber syndrome. It is an under-recognized, rather than a very rare, condition among patients with large facial hemangiomas. On the basis of a recent review of 327 patients with hemangiomas of infancy, PHACE syndrome occurred in 3.36% of the patients with hemangiomas(5). Females are affected eight times as compared to males(6). The predominance of the female gender led to the speculation that PHACE syndrome might represent an X-linked dominant condition with lethality in males(7). It constitutes a spectrum of anomalies with majority of the affected cases (about 70%) having only one extracutaneous manifestation. The full spectrum of potential abnormalities in patients with PHACE syndrome is, yet to be described(5). Among the CNS abnormalities, Dandy-Walker malformation is most commonly noted. Cases with supratentorial abnormalities have been reported, including the absence of foramen lacerum, microcephaly, cortical dysplasia, frontal lobe calcifications, encephalomalacia, etc.(5). The hemangioma is usually large, segmental and distributed along trigeminal division V1 dermatome in 75% of cases. Most are left sided (43%), occasionally right sided (29%) and bilateral lesions (27%) are seen. Extracutaneous hemangiomas were reported in 22% of cases. The subglottic airway was the most common location and was seen exclusively with cutaneous hemangiomas involving the mandibular region(8). Coarctation of aorta is the most common arterial anomaly. The cardiac lesions include patent ductus arteriosus, ventricular septal defects, atrial septal defects, pulmonary stenosis, cor triatriatum, tricuspid atresia and stenosis, tricuspid aortic valve and tetralogy of Fallot. Other aortic anomalies include aberrant origin of the subclavian artery, subclavian or innominate artery aneurysms, ascending aorta or aortic arch aneurysms or dilatation, anomalous left superior vena cava, congenital valvular aortic stenosis, hypoplastic descending aorta, and double aortic arch and double aortic coarctation(8). Ophthalmologic manifestations occur in 20% of cases. These include retinal vascular abnormalities, optic atrophy, iris vessel hypertrophy, iris hypoplasia, morning glory disc, congenital cataract, sclerocornea, lens coloboma, and exophthalmus(9). Sternal clefting and supraumbilical raphe are ventral developmental defects associated with this condition. Subtle sternal defects like the presence of sternal pits without underlying soft tissue or bony loss may be observed. The presence of sternal clefting and/or a supraumbilical raphe was associated with a hemangioma involving the trigeminal division V3 dermatome in more than 90% of cases(8). The review of PHACES related symptoms published in 2001 by Metry et al comprised three cases of thyroid anomalies. Of the 130 cases reviewed, two had congenital hypothyroidism while one had lingual ectopic thyroid(8). Thyroid function screening of infants with either very large haemangiomas or hepatic lesions should be considered. Huang et al reported a 3-month-old infant with a massive hepatic hemangioma and primary hypothyroidism(10). Our case was diagnosed to have congenital hypothyroidism based on serum T4 and TSH reports done on the twenty-fifth day of life. Thus in patients presenting with a large facial hemangioma, it is important to conduct an attentive neurological examination completed by brain imaging and an extensive cardiovascular exploration. Special attention should be given to the ophthalmologic and sternal examinations as well as the search for hemangiomas in airway localization. Acknowledgement The authors thank Dr. (Prof) Maya Mukhopadhyay, Head of the Department of Pediatrics, The Institute of Child Health, Kolkata for providing all the support. Contributorst: AG Conception and design, SRT manuscript writing and design and RT data compilation and manuscript drafting. Funding: None. Competing interests: None. | ||||
|
References | ||||
|
|
![]()