|
|
Short Communication Indian Pediatrics 2007;44:133-136 |
||||||||||||||||||||||||||||||||||||||
|
Seroprevalence of Chlamydia pneumoniae in Asthmatic Children from Northern India |
||||||||||||||||||||||||||||||||||||||
|
From the Department of Pediatrics*, Advanced Pediatric Center and Department of Medical Microbiology, Post Graduate Institute of Medical Education and Research, Chandigarh, India. Correspondence to: Dr. Sunil Sethi, Assistant
Professor, Department of Medical Microbiology, Post Graduate Institute
of Medical Education and Research, Chandigarh 160 012, India.
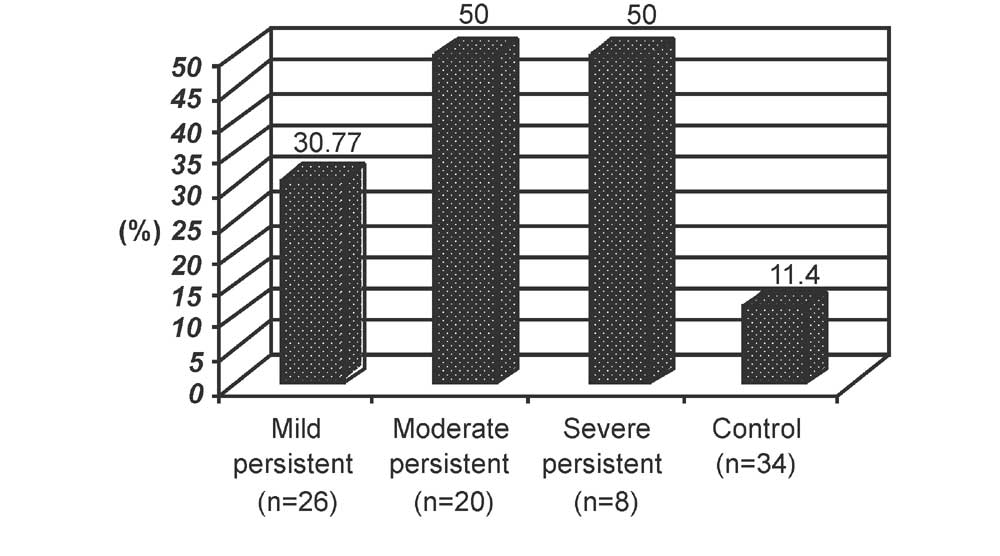
Abstract: Serum from children with chronic persistent asthma was subjected to C. pneumoniae IgG antibody determination. C. pneumoniae IgG serology suggestive of persistent infection was significantly higher in chronic persistent asthma group than in the control group. Seropositivity was significantly more in moderate and severe persistent groups than in the control subjects. There was no evidence of acute C. pneumoniae infection (IgM serology done in duplicate) in acute exacerbations. Key words: Chlamydia pneumoniae, Chronic asthma, Serology. C. pneumoniae has been shown to infect human smooth muscle cells(1), generate inflammatory cytokines in vitro(2) and has also been linked to asthma. Most of the studies evaluating association between C. pneumoniae and asthma have been done in adults(3-5). Information in children is scarce with most reports showing association with acute exacerbations of asthma(6-8). We evaluated the potential role of C. pneumoniae infection in chronic persistent asthma and acute exacerbation of asthma. Subjects and Methods Between January 2001 and February 2002, 54 children with physician diagnosed chronic persistent asthma (based on history, physical examination and lung function) and 10 children of persistent asthma with acute exacerbation in the age group of 5-14 years presenting to Asthma Clinic in PGIMER, Chandigarh were enrolled for the study. The subjects were categorized into different severity grades according to the NHLBI consensus guide-lines(9) into mild persistent (n = 26), moderate persistent (n = 20) and severe persistent asthma (n = 8). Children with immunodeficiency, connective tissue disease and other autoimmune diseases were excluded. Thirty four healthy children in the similar age group served as controls. Pulmonary function tests were measured by Spirometer (vitalograph) in the standing position and compared to the norms in relation to height for age and sex. 2 mL of the venous blood was collected from all asthmatic and control subjects. Detection of C. pneumoniae IgG antibody was carried out in all subjects {chronic asthma (n = 54) and chronic asthma with exacerbation (n = 10)} in duplicate. In addition, C. pneumoniae IgM antibody was studied only in children with acute exacerbation. Serum was separated by centrifugation, aliquoted and stored at –70°C and subjected to ELISA (Savyon diagnostic Ltd., Israel). Sensitivity and specificity of the above ELISA method is 95% and 97% when compared to the microimmunofloresence method (information provided by the manufacturer). Ethical committee of the hospital approved the study and samples were collected after obtaining written consent from the parents. Data obtained was compared using Chi square test with Yates correction and Fisher exact test. Results C. pneumoniae IgG titers consistent with persistent infection was found in 40.62% (26/64) of subjects whereas only 11.4 % (4/34) of the children in the control group had positive C. pneumoniae IgG antibody titers (p = 0.003). Further comparison of the C. pneumoniae IgG antibody in relation to the different severity grades of chronic asthma is presented in Fig 1. Presence of C. pneumoniae IgG antibody was significantly more in the persistent asthma as compared to the controls. None of the 10 patients with acute exacerbation of asthma showed a positive IgM C. pneumoniae serology in duplicate samples.
Mean selected lung functions in seropositive and seronegative patients of different severity grades disease severity were compared. Percentage predicted mean FEV1% (71.48(9.72 in mild persistent) and 63.00 ( 8.88 in moderate persistent asthma) and mean FVC % of predicted 76.88 ( 9.53 in mild persistent and 68.50 (9.46 in moderate persistent group) were much lower in seropositive group as compared to seronegative patients (Table I). Those with severe persistent disease showed no difference with seropositivity for Chlamydia. TABLE I Selected Lung Function in Different Severity Grades of Asthma in Subjects With and Without Positive Serology
Discussion The results of our study showed that C. pneumoniae IgG antibody titer suggestive of persistent infection was significantly more in children with chronic persistent asthma as compared to the controls and association was significant for moderate and severe persistent groups. Several studies in adults have shown the association between the presence of C. pneumoniae IgG antibody seropositivity and chronic persistent asthma(10,11). That seropositivity represents true infection has been shown in couple of studies using PCR and serology together(12,13). Possible mechanisms to increase the severity of chronic asthma may be the result of increased production of inflammatory cytokines(1,2). The present study also suggests that C. pneumoniae IgG seropositivity was associated with impaired lung function. Strachan, et al.(14) showed no evidence of association between C. pneumoniae IgG antibody and decline of pulmonary function in adult patients with chronic obstructive pulmonary disease and asthma. No evidence of rising titer of IgM C. pneumoniae antibody suggestive of acute C. pneumoniae infection was found in acute exacerbation of asthma. Our study shows association between C. pneumoniae IgG seropositivity and chronic asthma especially the more severe forms of asthma. If the results of this study are replicated by a larger study then children with persistent asthma symptoms could be considered for evaluation of C. pnuemoniae IgG and treatment.
| ||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||
|
| ||||||||||||||||||||||||||||||||||||||
![]()