|
|
Original Article Indian Pediatrics 2006; 43:125-130 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Prediction of Weight of Indian Children Aged upto Two Years Based on Foot-length: Implications for Emergency Areas |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sandeep B. Bavdekar, Shefali Sathe and Pranav Jani From the Department of Pediatrics, Seth G.S. Medical College and K.E.M. Hospital, Parel, Mumbai 400 012, Maharashtra, India. Correspondence to: Dr. Sandeep B. Bavdekar, Flat Number 9, A2 Worli Seaside CHS, Pujari Nagar, KAG Khan Road, Worli, Mumbai 400 018, Maharashtra, India. E-mail: [email protected] Manuscript received: April 20, 2005; Initial review
completed: June 15, 2005;
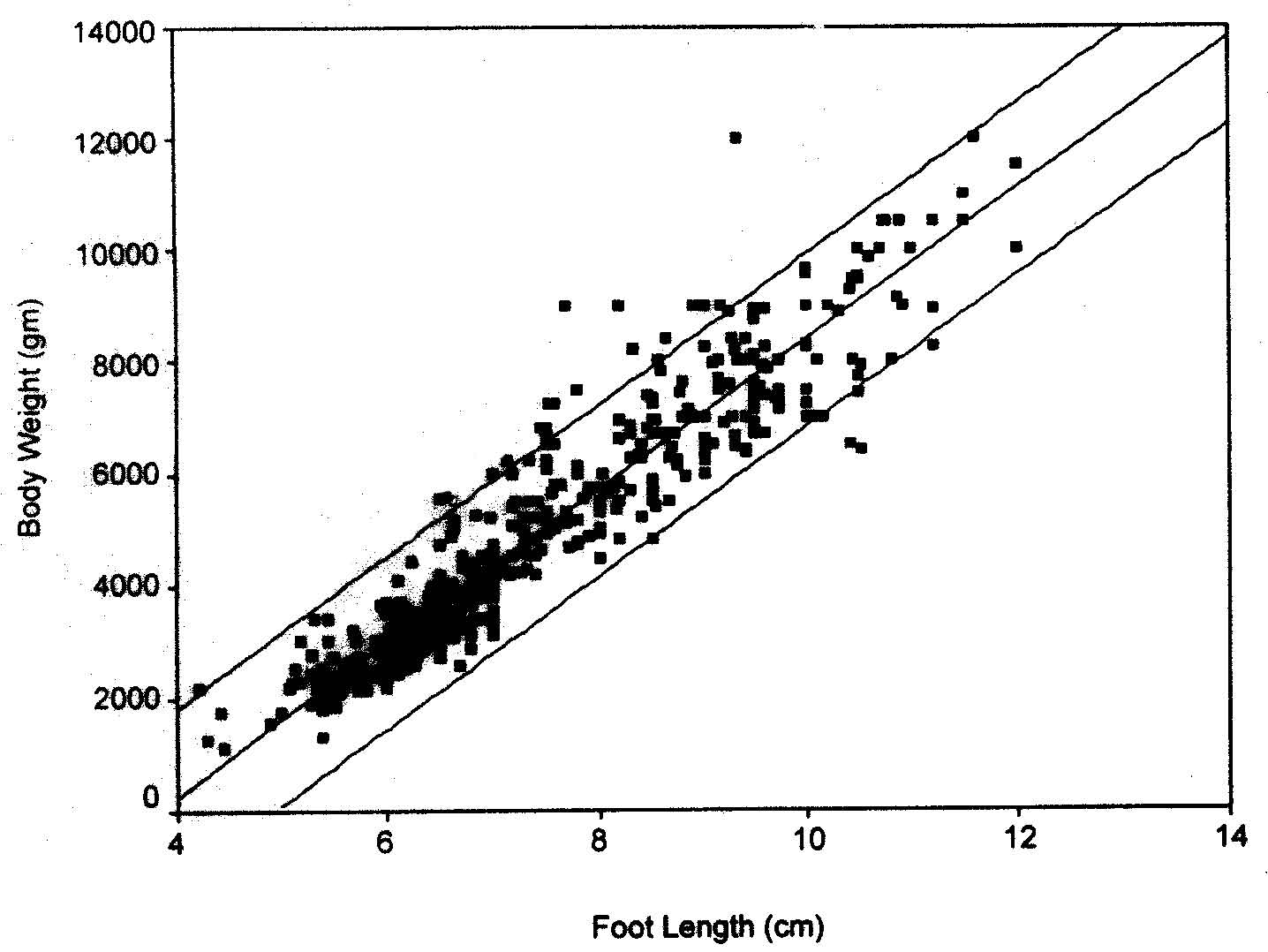
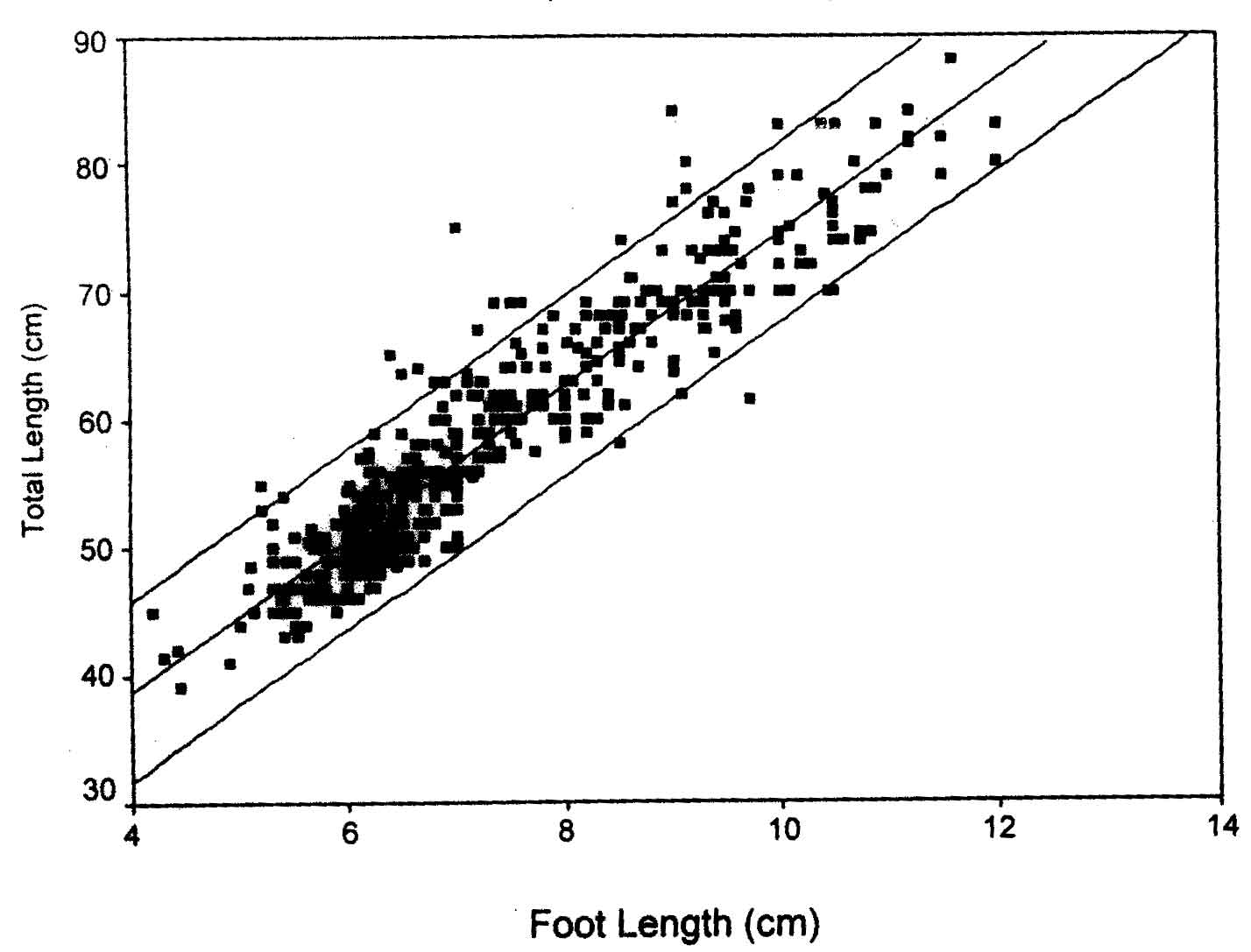
Background: Children presenting in critical care department might receive improper drug doses, as their weight and length cannot be determined while they are being resuscitated. Aims: To determine if there is a correlation between foot-length and weight, length and surface area and to compare the drug doses calculated as per predicted weight (determined on the basis of foot-length) with those calculated on the basis of actual weight. Material and Methods: Weight, length and foot-length of children aged up to 24 months were determined in the prospective study. Analysis was done using simple linear regression analysis and by determination of coefficient of determination. The dosages of emergency medications (epinephrine, atropine, Ringer’s lactate and diazepam) were calculated on the basis of actual weight and dosages given in standard text and were then compared with dosages likely to be administered on the basis of weight predicted by foot-length measurement. Results: Five hundred subjects were enrolled in the study that demonstrated a significant linear relationship between foot-length and body weight (r2 = 0.88, p<0.01), total length (r2 = 0.88, P<0.01) and body surface area (r2 = 0.84, P<0.01). The weight could be predicted on the basis of the following formula: Weight (kg)= –5.15 + [1.35 × foot-length (cm)]. The doses of drugs calculated on the basis of weight predicted from foot-length were exceeded the standard dose by 2.35-2.40%. Conclusions: In children aged up to 2 years, foot-length can be used to predict weight and calculate doses of emergency drugs. Keywords: Anthropometry, Critical care, Infant, Foot-length, Surface area, Weight. When children present in a critical condition, resuscitative measures are employed immediately. The patient gets surrounded by doctors and paramedics, who immediately begin processes such as quick clinical evaluation, securing intravenous access, administration of oxygen and at times undertaking endotracheal intubation, cardiac massage and cardioversion. Under such circumstances it is not feasible to determine child’s weight, length or surface area; the three parameters that are commonly used for calculating drug doses. It was hypothesized that even when a patient is surrounded by ICU personnel and various machines, it would still be possible for the paramedics to determine the patient’s foot-length. In addition, previous studies done in the neonates have shown that foot length can be used to predict birth weight, length and naso-tracheal tube length(1,2). Hence, a study was undertaken to check if footlength correlates with weight, length or surface area, to devise a formula for prediction of weight based on foot-length observed and to ascertain if drug doses calculated on the basis of predicted weight conform with usual doses. Subjects and Methods The study was carried out in the Well-Baby clinic, pediatric outpatient department and wards of a large tertiary care hospital over a period of 6 months, after obtaining clearance from the Institution’s Ethics Committee. For the purposes of estimation of sample size for the study, a pilot study was initially carried out in 20 patients and a linear regression equation was plotted and the values of slope and intercept derived. The value of the derived slope with a standard deviation of 0.33 for the independent variable and 0.4 for the dependent variable using the method of Dupont and Plummer gave a sample size of approximately 500 patients for the final study at 80% power and 5% significance(3). Consecutive children aged up to 24 months were enrolled in the study after obtaining written informed consent from parent or lawful guardian in a pre-designed consent form. The subject’s age was determined on the basis of birth card or birth certificate. The details such as birth weight and gestational age at birth were recorded. In infants aged 6 months or below, history of feeding was asked for. The feeding patterns were designated as exclusive breastfeeding, almost exclusive breastfeeding, mixed feeding and exclusive top feeding(4). For categorization, feeding history in the last 24 hours was considered(4). Single investigator (SS) took the anthropometric measurements (weight, length and footlength) so as to avoid inter-observer variation. The weight was recorded on an electronic weighing scale (Zeal India Limited, maximum capacity 20 kg, least count 5 g) by bringing the digital display of the scale to hold(5). An infantometer with a least count of 1 cm was used for determining the child’s length(5). The foot-length was recorded with the help of metallic Vernier’s calipers (least count 0.01cm)(1). The data was analyzed using linear regression analysis. Attempts were made to derive formulae that would predict weight on the basis of footlength. The coefficient of determination (r2) was calculated. Mean dosages of the emergency medications (namely epinephrine, diazepam, Ringer’s lactate and atropine) obtained from standard pediatric texts were used for comparison(6,7) between doses calculated as per actual weight and those calculated on the basis of predicted weight. Results Five hundred subjects (263 boys, 237 girls; M: F ratio being 1.11:1) were enrolled in the prospective study carried over a period of 6 months. As shown in Table I, the maximum number of study subjects were in the post-neonatal age group. Twenty-six (5.2%) subjects were born preterm while the rest were born at term. Three hundred and twenty-three (64.8%) subjects were exclusively breastfed and 141 (28.2%) subjects were mixed fed. All the 150 neonates and 57.3% of infants in the post-neonatal age group were exclusively breastfed. In infancy, 106 (35.1%) babies were receiving mixed feeds. Figure 1 demonstrates a significant linear relationship between foot- length and body weight (r2 = 0.88, P <0.01). The coefficient of determination of 0.8838 indicates that 88% of the variability in weight might be explained by the linear regression model. There also exists a significant linear relationship between foot-length and total length (r2 = 0.88, P <0.01) (Fig. 2) and between foot-length and body surface area (r2 = 0.84, P <0.01). Using the data available, investigators also performed simple linear regression analysis between the outcome variable, viz., weight and independent variable, i.e., footlength. Using the best-fit regression line, a mathematical formula was derived for prediction of weight (g) based on foot-length (cm): Weight (g) = –5.15 + [1.35 × foot-length (cm)]; where –5.15 is the constant. Table II depicts the relationship between the standard dose (mg or mL per kg) given in the pediatric texts and the mean predicted dose in terms of actual weight (mg or mL per kg). It was found that the dose of drug administered on the basis of actual weight of the child is similar to the dose that would be administered if weight predicted on the basis of foot length were to be used. The dose calculated on the basis of predicted weight exceeded the standard dose by 2.35-2.4% for the drugs studied. Table I
Figures in parentheses indicate percentages
Table II
Figures in parentheses indicate 95% confidence interval, * Doses in mL or mg/kg actual weight.
Discussion When a child presents in a critical condition, it is not possible to move the child to a weighing scale for determination of body weight. Although, drug doses can be calculated on the basis of total length(8), measuring length is also fraught with problems due to limited accessibility to the patient, who gets surrounded by machines and by doctors and paramedics undertaking various diagnostic and therapeutic procedures. Under such circumstances, doctors either look for the record of pre-morbid weight or predict weight on the basis of age or observed stature. Doctors working in intensive care units of public hospitals in developing countries have additional problems: As children do not visit their doctors regularly, their recent weight record (pre-illness weight) is not available. Also, most parents do not necessarily keep the medical records diligently. Predicting weight on the basis of chronological age is also fraught with dangers due to the presence of rampant moderate to severe malnutrition in our community. This makes use of standard percentile charts (NCHS) for determination of weight redundant(9,10). Measuring foot-length is possible even when the child is in a critical state: Foot remains away from the main theatre of activity and is, therefore, easily accessible. Foot-length can be easily measured using a Vernier calipers, which is neither costly nor is it technically challenging to use. In addition, there is no need to shift the patient or put him in a particular position for the determination of foot-length. This study has shown that foot-length correlates with anthropometric parameters such as weight, total length and body surface area; the parameters that are used to determine drug doses in children. The study also demonstrated that weight could be predicted on the basis of observed foot-length and that the doses calculated on the basis of this predicted weight exceeds standard dose by only 2.35-2.4%. Armed with these findings, the intensive care units could now put up charts that would depict (expected) weight and even drug doses calculated on the basis of predicted weight (Table III). This would ensure that children presenting in an emergency receive optimum doses of medications. Table III
ADR: Adrenaline, ATR: Atropine, DZ: Diazepam, RL: Ringer’s Lactate.
We enrolled children up to the age of 24 months, as they constituted over 40% admissions to the pediatric intensive care unit at our institution. It is true that we did not select patients actually admitted in the IPCU, as it would have taken enormously longer duration to enroll 500 subjects. We assumed that children who attend the pediatric outpatient wards, well baby clinics and Indoor services were the ones who would visit the hospital in case of an emergency. Thus, the sample collected from these areas of the hospital would be representative of patients accessing the hospital’s intensive care and emergency services. The importance of the study for emergency and intensive pediatric care units cannot be overemphasized. It provides health care providers with an easily measurable parameter for estimation of weight and through it estimation of dosages of at least the emergency drugs. The question that may come up is whether the study sample is representative enough to be used in all children from resource poor countries or even all the Indian children. The entire sample was drawn from children attending a public hospital. Children who come from socially and economically disadvantaged sections of the society use the services in the hospital and hence our sample may not represent those belonging to the higher strata of the society. However, it is likely to be representative of children living under similar conditions and we are sure that this would account for a vast majority of children availing the services of intensive care units and emergency services of public hospitals in resource-poor countries. The details of gestational age and feeding pattern provided in the text would help other healthcare providers to judge for themselves, if this data could be directly applied to their settings. Even if this formula cannot be directly applied, the idea of using footlength to predict weight and doses of emergency medications is still valid and a similar study on pilot basis could help deduce the right formula for each setting. Acknowledgments Authors thank Dr. Nilima Kshirsagar, Dean, Seth GS Medical College and KEM Hospital for permitting them to publish this article. They are also grateful to Dr. Nithya Gogtay, Associate Professor of Clinical Pharmacology, Seth GS Medical College and KEM Hospital for providing vital inputs in the finalization of the manuscript. Contributors: SBB: concept and design and supervision of data collection, revision and fianalization of the draft and act as guaranter of the manuscript; SS: collection, analysis and interpretation of data, preparation of the first draft; PJ: Collection of the data and assistance in revision of the first draft. Funding: None. Competing interests: None.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
|
![]()