|
|
Letters to the Editor Indian Pediatrics 2005; 42:188-189 |
||
|
Acute Lead Encephalopathy with Optic Neuropathy |
||
|
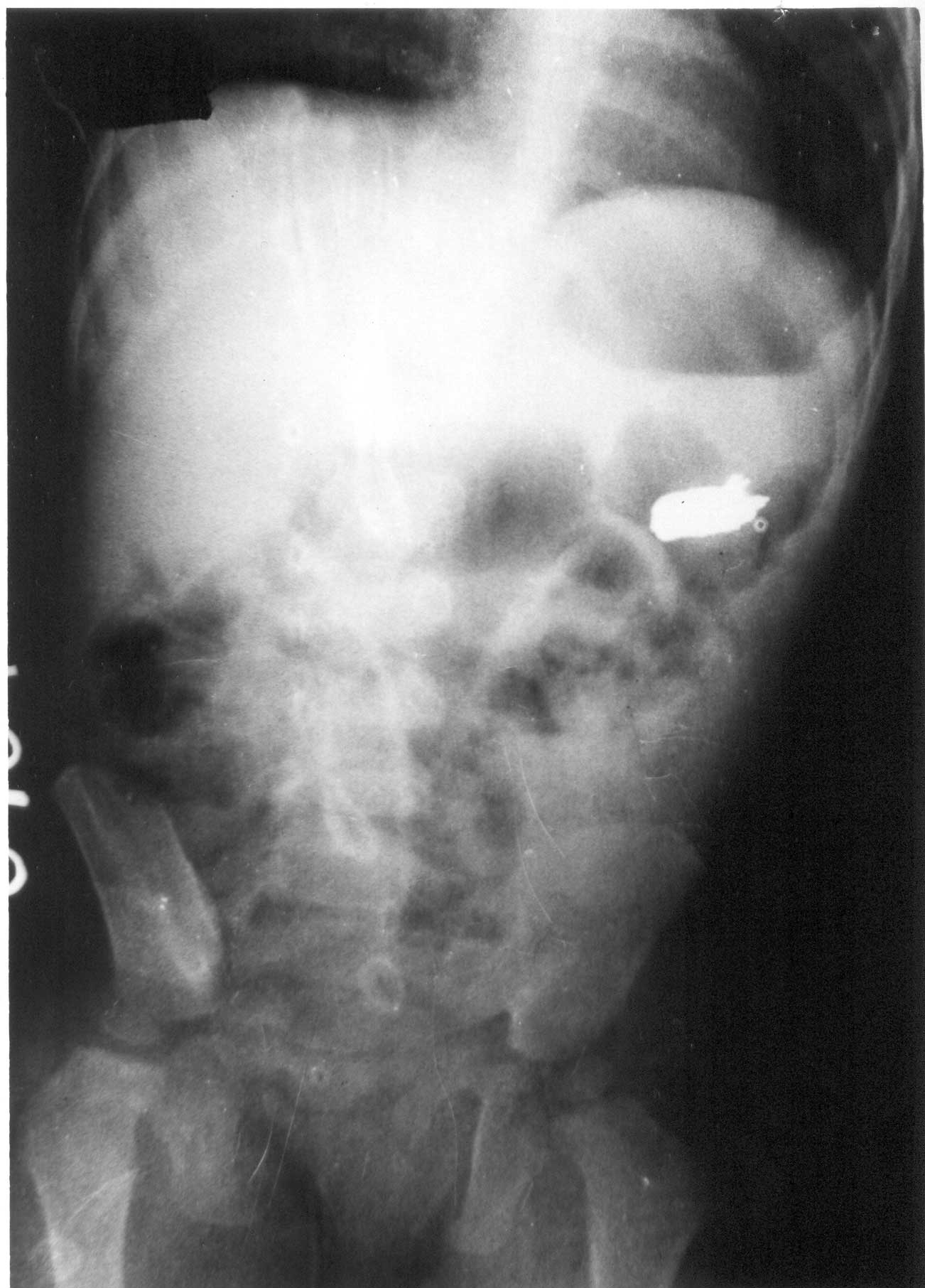
An 11-month-old girl was brought with a history of ingesting a metallic object used for fishing, 15 days prior to admission. She had fever, vomiting, constipation for 3 days, convulsion and absence of menigeal signs or neurological deficits. She had normal fundus, cerebrospinal fluid (CSF), total and differential leukocyte counts and normocytic hypochromic anemia (Hb 8 g/dL). Plain radiograph of the abdomen revealed a radio-opaque foreign body of size 0.5 × 1.5 cm in left hypochondrum, which was subsequently not observed in the stool (Fig. 1). On 4th day of hospitalization she developed signs of raised intracranial tension and then lapsed into shock. The serum electrolytes were normal and the CSF remained normal. Blood was withdrawn for lead levels that were 129 µg/dL by flameless atomic absorption spectro-photometry. She was treated with D-penicillamine (30 mg/kg/day), the only available chelator in the market. She was also given supportive treatment for raised intracranial tension with shock. Within 48 hours there was an improvement in her sensorium and her vital parameters stabilized. However, fundus examination on the 8th day revealed anterior ischemic optic neuropathy. Her blood lead a week later was 67 µg/dL.
This was a patient of acute lead poisoning encephalopathy resulting in ischemic optic neuropathy, rare neurological sequelae. The combination of raised intracranial pressure and anemia is responsible for ischemic optic neuropathy in lead encephalopathy(1). Existing high prevalence of iron deficiency anemia may increase the toxic effects of lead on children in our country(2). The prevalence of elevated blood lead level ( ³10 µg/dL) in preschool children in the community has been reported to be 67.7% in this city, the main sources of exposure being house paint and eye cosmetic (surma)(3). Acute lead encephalopathy is an emergency usually resulting from ingestion of lead rich objects and associated with blood 1ead ³100 µg/dL(4). Because of this high prevalence of elevated lead levels in the community, the possibility of lead encephalopathy should always be considered in the differential diagnosis of children presenting with coma and convulsions of unknown etiology, and, blood lead levels should be obtained even in absence of history of ingestion of lead rich objects. Even when identified and promptly treated, severe and permanent brain damage may result in 70-80% children(5). Prompt recognition of prodromal symptoms followed by early medical management with chelating agent can prevent the onset of life threatening complications. Archana Patel,
| ||
|
References | ||
|
|
![]()