|
|
Brief Reports Indian Pediatrics 2005; 42:134-139 |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Sexual Abuse of Street Children Brought to an Observation Home |
||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Deepti Pagare, G.S. Meena, R.C. Jiloha and M.M. Singh From the Departments of Community Medicine and
Psychiatry, Maulana Azad Medical College, Correspondence to: Dr. Deepti Pagare, C-601, Kalka
Apartments, Sector-6, Plot no. 31, Manuscript received: December 2, 2003, Initial
review completed: January 6, 2004;
Sexual abuse of a child is defined as, "the involvement of a child in a sexual activity that he or she does not fully comprehend, is unable to give informed consent to or that violate the laws or social taboos of society"(1). WHO estimates that globally, 8% of boys and 25% of girls below age 18 are estimated to suffer sexual abuse of some kind every year(1). A community based multi-centric qualitative study revealed that sexual abuse of children in India crosses all barriers of socio-economic classes and is widespread among both rural and urban areas and among boys and girls(2). Abusive practices were found to range from traditional systems like "Besavi" and "Vardiyar " to well organized sex trade in Mumbai, Delhi and Goa. Sexual abuse has been reported by domestic and agricultural labor(2) as well as educated high school students(3). Some clinic-based studies have also documented sexual abuse(4,5). Perpetrators of sexual abuse find their victims in wide ranging situations and it is natural that homeless boys, living in unprotected environment on streets make easy prey for sexual abuse, as evidenced by many studies(6-9). Under the Indian Juvenile Justice Act (JJA), 1986 (modified 2001), these boys are temporarily kept in observation homes(10). The present study attempts to ascertain the magnitude of sexual abuse suffered by inmates of an observation home in Delhi before admission. Subjects and Methods The study was conducted at an observation home for boys in Delhi where non-delinquent male juveniles aged 6-18 years are temporarily detained. All the boys admitted for the first time to observation home between May to October 2002 were included. Each child was individually approached by the interviewer as soon as possible after admission and was first interviewed regarding his socio-demographic profile. An attempt was made to classify the socio-economic status of the participants with the help of a self-developed scale selecting parameters, the information regarding which was likely to be provided by the children, without validation from parents(11). After this, each participant was interviewed regarding any episode of sexual abuse recalled by child anytime before admission. Any number of episodes reported by a child was recorded as a single entry. Sexual abuse was measured using two standardized scales namely the Finkelhor’s scale(12) to assess the detailed nature of the sexual act and the Child Maltreatment History Self- Report(13) to calculate the proportion of sexual abuse among the subjects. The scales were translated in Hindi, re-translated in English and pre-tested on thirty inmates of the observation home in March and suitably modified. The results of pilot study were not included in the analysis as it was carried out on old inmates of the observation home. Following the interview, the boys were requested to undergo examination in a separate room by the medical officer of the observation home, based on the guidelines of American Medical Association (AMA, 1985) for primary care physicians for diagnosis of suspected sexual abuse(14). The ethical committee of the medical college and the observation home authorities approved the study. All the boys were assured confidentiality and none was forced to undergo physical examination against his will. Privacy was maintained during interview and examination. Anonymity was maintained throughout data processing and analysis. Results A total of 202 boys willing for clinical examination were enrolled. Thirteen were excluded because of IQ < 70 (n = 7) and inability to understand either Hindi or English (n = 6). The final sample consisted of 189 boys. Majority of subjects belonged to urban, Hindu nuclear families and lower or lower middle socio-economic classes. Among the 178 subjects living away from families, 62.9% had left home between 6 to 10 years of age (mean age at leaving home; 9.03 ± 2.5 years). Eleven boys could not provide complete information for socio-economic status and were excluded from analysis. The various acts of sexual abuse are presented in Table I. Overall, 38.1% boys reported sexual abuse with use of force ranging from 4.8% to 23.8%. Over 15% boys reported penetrative sexual abuse. The maximum proportion of abuse was reported in the age groups 8-10years (42.9%). Table I Nature of sexual abuse experienced by study subjects (N = 189).
* The responses are not mutually exclusive. ** Only one subject reported sexual abuse by a female perpetrator. The mean age at abuse was reported as 9.13 + 2.4 years. Most children (93.2%) reported the incident to be within 2-3 weeks of leaving home. The mean duration between the incident and interview was 2.34 + 0.4 years. All boys reported single episode of sexual abuse except four. The maximum proportion of incidents occurred during late evening or night (59.2%). In 22.2%, the episode occurred during day. Most children (76.2%) were abused at the railway platforms, commonly in some deserted or empty railway coach. About 4% were abused at the work place and 1.4% at some other observation home.
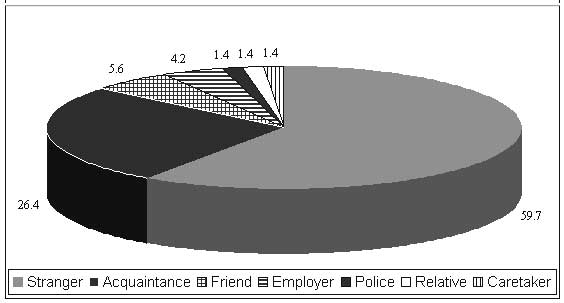
Figure 1 shows the most common perpetrators to be strangers followed by some acquaintance (26.3%). All the perpetrators were males except for one. Table II shows that among the 72 abused children, 44 (61.1%) had some physical sign of abuse while 29 (40.2%) showed behavioral signs of sexual abuse. Eighteen boys presented with signs suggestive of sexually transmitted diseases. Table II Signs of sexual abuse observed on examination of study subjects as per AMA guidelines (N = 189).
*History of recurrent urinary tract infections has been considered an important sign suggestive of sexual abuse in children by American Medical Association.
Discussion The present study attempts to explore the traumatic experiences of sexual abuse among homeless boys in Delhi. Much work on sexual abuse has been devoted to the girl child(2) neglecting the equally important issue of the male sexual abuse. Most street children are males(6) and are at higher risk of abuse on streets. More than one third of boys reported sexual abuse in the present study. Other studies on general population have reported rates of sexual abuse, ranging from 0.6%(15) to 29%(12) among males. The lack of use of uniform definition for categorizing sexual abuse can account for difference in reported rates(16). Studies on homeless boys have reported comparable rates of sexual abuse(7,8). In the present study, many victims were
threatened with knife and blades similar to other studies (7,8). The
use of force may result in extensive injuries to victims’ genitalia,
which facilitate transmission of sexually transmitted diseases
(STDs) as revealed during clinical examination by presence of
genital wounds in 14% of victims and signs suggestive of STDs in
25%. These signs are important corroboration of self-reported sexual
abuse(4,14,17). The presence of STDs, homosexual nature of abuse and
evidence of trauma also raises concern regarding increased
vulnerability of these children to HIV infection(6,17,18). The most
common abusers were strangers, similar to other Since the child may not know his age properly, the age presented in results is based on the official records of the observation home authorities, determined by the Child Welfare Committee at the time of initial presentation. The limitation of the present study is that the traumatic experiences of abuse may have been underreported or exaggerated depending on the individual characteristics of the children. The study may have missed the very early childhood experiences of sexual abuse, forgotten by the child. Some of the signs may get modified or may disappear during the course of time. However, the study gives an insight into the vulnerability of street children for sexual abuse. The clinical examination provides supports the self-reports of children. Finally, it can be concluded that the problem of sexual abuse among inmates of observation home is grave and requires urgent remedial action. The period of detention at observation homes may be utilized for identification of the victims and their proper medical, social and psychological rehabilitation to prevent further abuse. The World Health Day theme for the year 2003 wass "Safe environment for children" which also envisages appropriate action by the concerned authorities to make efforts in creating safe living conditions of all children including street children. Acknowledgements The authors gratefully acknowledge Dr. Pranay Bhanu, Medical officer and staff of "Prayas" observation home for boys, New Delhi, Mr. Rajan Gupta, Clinical child psychologist, Lok Nayak hospital and the interns from the batch of 2002, Maulana Azad Medical college, for their active support and co-operation for this research. Contributors: DP developed the concept and design of the study, collected the data, analyzed, interpreted the data and wrote the draft and final paper. GSM and RCJ revised the draft and gave approval of the version to be published. MMS helped in conceptualizing and designing the study, analysis and interpretation of the data, drafting and revising the article. Competing interests: None stated. Funding: None.
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| ||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
![]()