|
|
Recommendations Indian Pediatrics 1999; 36:157-165 |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
Consensus Guidelines on Management of Childhood Asthma in India |
|||||||||||||||||||||||||||||||||||||||||||||||||||||||||
Asthma is a common disease amongst children in India with prevalence estimated at 5-10%. A world wide increase in the prevalence of
asthma is being reported with increase in wheeze at an alarming rate of 5% per year. From 1983 onwards an increase in asthma mortality and morbidity has been noticed globally(1). Several guidelines have been published since 1990 with the aim of improving management of asthma. However, a systematic analysis of guidelines till 1995 had brought out several controversial issues as well as gaps in knowledge(2). In May 1997, guidelines were published about management of asthma by an Expert Committee of the National Heart Lung and Blood Institute of USA where they tried to overcome many of the previous lapses(3). The need for similar guidelines has always been felt amongst the physicians managing children in India. It is felt that the guidelines originating in this country would have much more relevance to the ground situation and the status of health services. Thus, to set up the process of achieving consensus towards suitable guidelines, a Consensus Conference was held on April 17 and 18, 1998 at the Advanced Pediatric Center of the, Post Graduate Institute of Medical Education and Research, Chandigarh in
which experts (Annexure I) who manage asthma patient and have published papers in this field, participated. These guidelines were also later endorsed by the Indian Academy of Pediatrics, Respiratory' Chapter. Recent evidence was accessed using' searches on Medline, Embase, Index Medicus and Excerpta Medica. Some of the contentious issues were resolved with the help of the Cochrane Library(4). Since the consumer of health care in India is not sufficiently literate, physicians have been assigned a lot of responsibility in decision making for the patients. The guidelines are required to be updated periodically and provide flexibility to individualize patients. Since in large areas in our country all the recommended modalities may not be available, suitable improvisations must be made. A child with asthma is to be monitored for
clinical signs and symptoms of asthma with the help of asthma diary given to the patients/ parents and record of peak expiratory flow rate with a standardized peak flow meter (Table
1). PEFR must be monitored at the physician's office, asthma clinics (where spirometry should be available) and in the emergency room. Patients with chronic severe asthma must be encouraged and trained to monitor their PEFR at home once a day routinely and twice a day if the morning reading is abnormal, to determine their PEFR variability. Patient's personal best should be assessed and used subsequently. Spirometry has been kept optional and emphasis must be given to patients's quality of life. Emphasis must be on self management but physician supervision must still be the primary mode. Patients must be given a written crisis management plan where literate; otherwise verbal communication at each contact must continue. TABLE I Basic Steps for Using a Peak Flow Meter
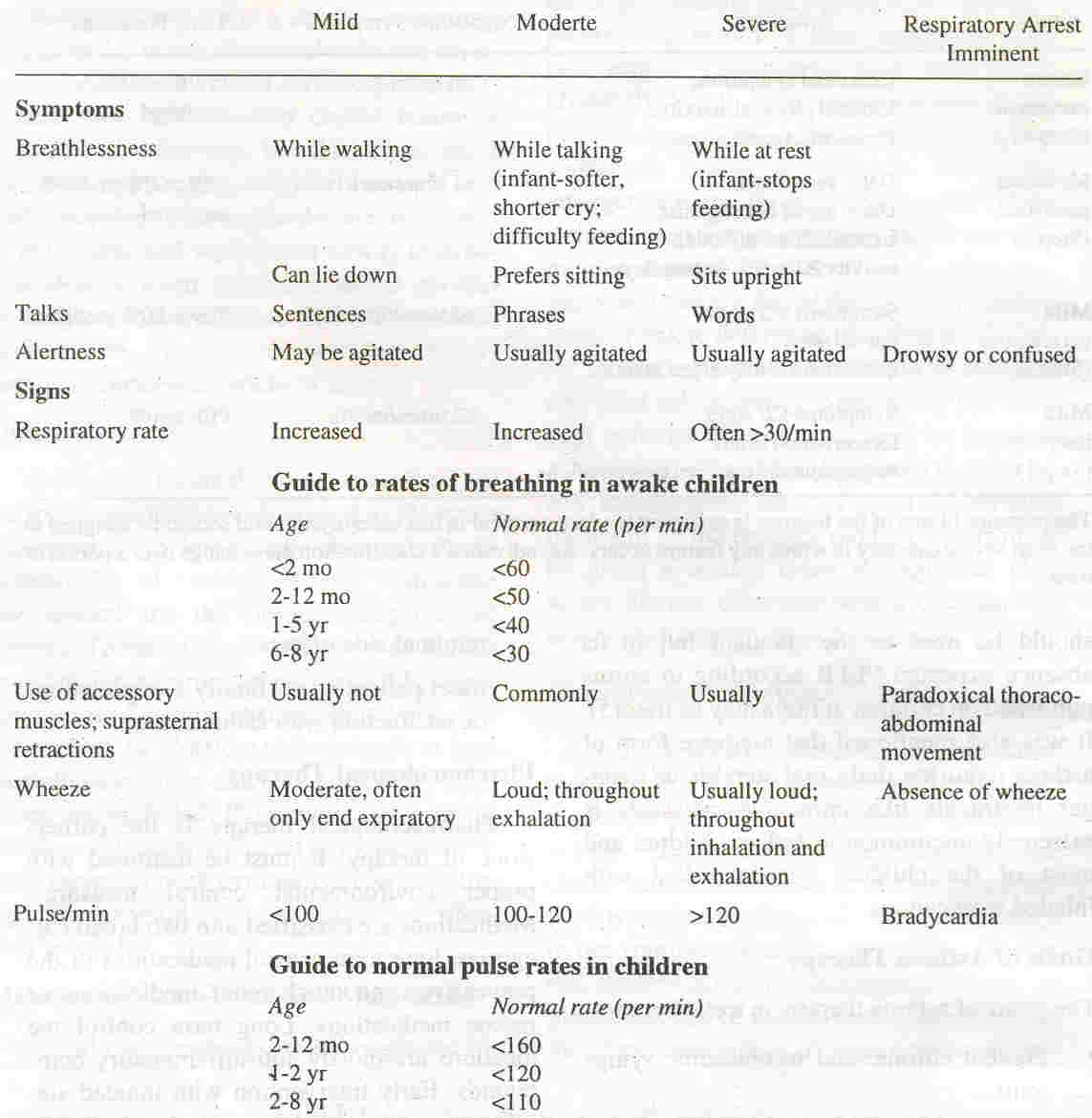
TABLE II Classification of Asthma Severity
TABLE III Classifying Severity of Asthma Exacerbations
Goals of Asthma Therapy The goals of asthma therapy in a child are to:
Pharmacological Therapy
Pharmacological therapy is the corner- stone of therapy. It must be
instituted with proper environmental control measures. Medications are
classified into two broad categories, long term control medications or the preventives and quick relief medications or rescue medications. Long term control medications .are mostly anti-infIammatory compounds. Early intervention with inhaled steroids can improve asthma control and normalize lung function and preliminary studies show that it might prevent irreversible airway injury. These are
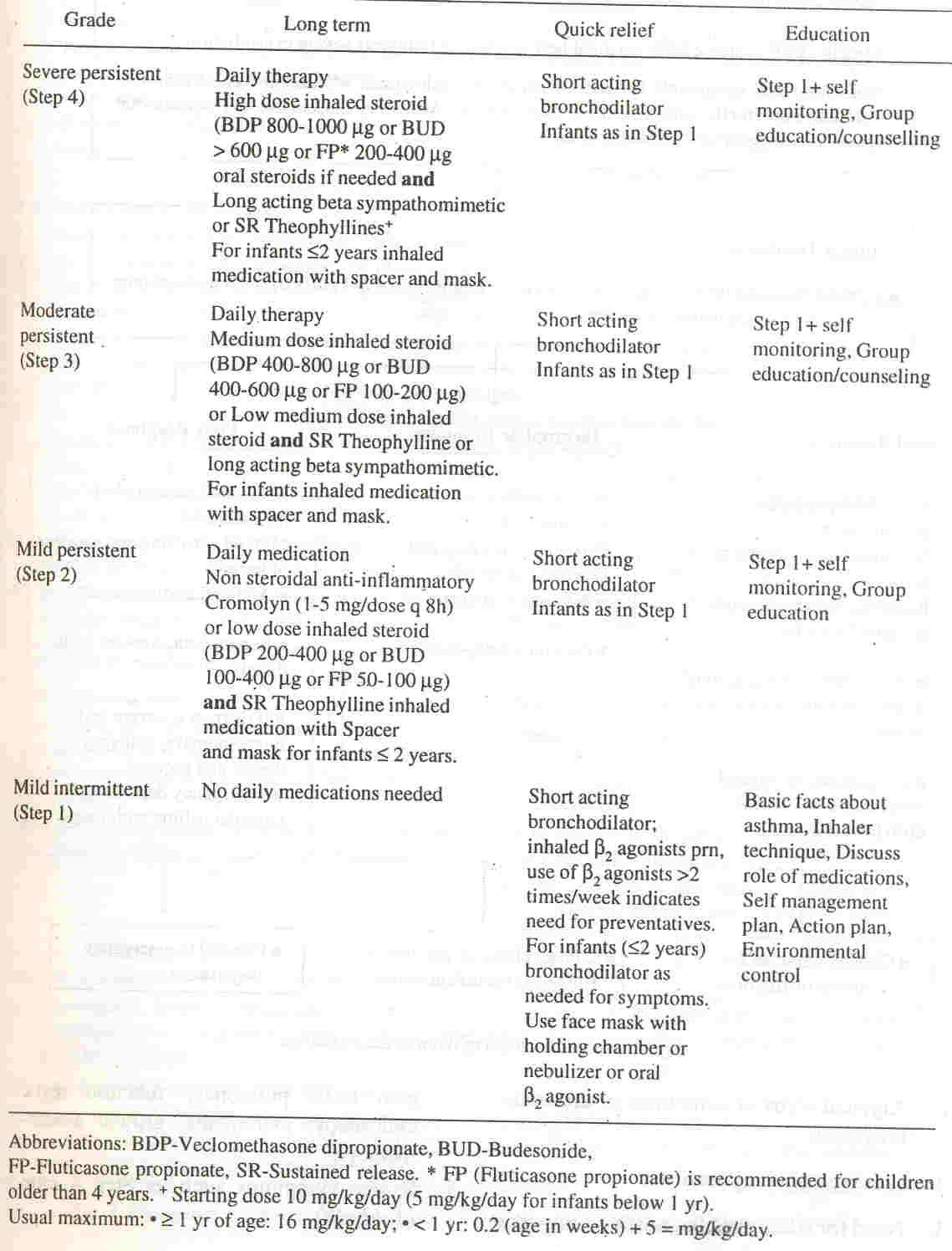
to be administered with the help of a metered dose inhaler and a spacer (in patients who cannot afford the commercially available spacers, a home made spacer can be used). Another alternative available in India is a dry powder inhaler (transparent rotahaler). Table IV Stepwise Approach in Long Term Management of Children with Asthma
Referral 2. Atypical signs or symptoms or uncertain diagnosis. 3. Presence of complications. 4. Need for additional diagnostic testing like skin tests, pulmonary function tests, endoscopy, incremental growth assessment, etc. 5. Severe symptoms such as step 4 care (Table IV). 7. Need for good asthma education. 8. Significant psychosocial or psychiatric problems.
Environmental Control and Prevention of Asthma Indoor Allergens Cockroach, house dust mite, fungal spores, animals (pets) are the main source. Skin testing can be used for the diagnosis. The following control measures are suggested:
Cockroaches: Leave no food uncovered. Traps to catch cockroaches are better than antiroach chemicals.
Pets: Pets like dogs, cats or birds should not be kept by children with asthma. Cats are not a common pet in India. Reports on pets are very few in this country. If pets are already in the house, contact with the patient should be minimized; or they should be kept out of the living premises. Seasonal exposure to pollens and fungi can be reduced by keeping the doors and windows closed from early I1!Orning till evening during the high pollen season. Air conditoning can be used. The filter of the air conditioner should be properly maintained.
Incase an allergen is found to contribute significantly to patient problem, he should be referred to a specialist for skin testing and if required, for immunotherapy, only if the child is not responding appropriately to pharmacotherapy and allergen is significantly contributing to disease.
Breastfeeding
Psychosocial Aspects of Asthma Management The experts stressed the need for health education not only in Asthma Clinic or Hospital but also on TV, Radio and other communication
media. The attitudes and practices concerning this disease demonstrate
a high degree of ignorance and misinformation. Written material containing information regarding basic facts of asthma should be made available to the patient and the parent while making the diagnosis. Special measures were recommended to be taken to educate the people
about the harms of passive smoking. The data presented indicate gross inadequacy of information regarding basic facts of asthma to patients and their parents. Intervention in the form of written material significantly improves the knowledge, of these individuals.
More studies need to be done to assess the knowledge attitudes and practices of these patients and specific materials developed
to improve the baseline information and change attitudes towards
inhalation therapy. Participants felt that there was a social stigma
attached to the disease and parents of the patients were specially concerned about the in-halation therapy having potential for producing drug dependence. More data needs to be generated towards epidemiology of asthma in this country especially as to why the incidence of asthma is relatively less in India and the disease is less severe as compared to some of the western
countries. The utility of yogic breathing exercises and role of Ayurved also needs to be evaluated. ANNEXURE I - MEMBERS OF THE CONSENSUS GROUP D. Behara, Anil Bhalla, Krishan Chugh, S.K. Gambhir, S.K. Jindal, S.K. Kabra, Lata Kumar (Convener), Keya Lahiri, Prabhjot Malhi, Uday Nadkarni (did not attend the Conference but participated in drafting the Consensus Guidelines), H. Paramesh, Sujeet Rajan, G.R. Sethi, Meenu Singh, Sunit C. Singhi. Rapporteurs for the Sessions: R.M.P.L. Ramanathan, K.O. Singh Writing Group: Meenu Singh, Lata Kumar, R.M.P.L. Ramanathan.
| |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|
References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||
1 Lewis S. ISAAC. A hypothesis generator for asthma? Lancet 1998; 351: 1220. 2. Meijer RJ, Kerstjens HAM, Postma OS. Comparison of guidelines and self management plans in asthma. Eur Respir J.1997; 10: 1163-1172. 3. Sly RM. New guidelines for - diagnosis and management of asthma. Ann Allergy Asthma Immunol1997; 78: 427-437. 4. The Cochrane Library: Update Software, Ox- ford, UK. 5. Parmar Y, Kumar L, Malik SK. Normal values of peak expiratory flow rate in healthy north Indian school children 6-16 years of age. Indian Pediatr 1977; 14: 591-594. |
![]()