|
|
|
Indian Pediatr 2019;56: 1083 |
 |
Lip Smacker’s Cheilitis
|
|
Abheek Sil1
and Pallavi Priyam2
Departments of 1Dermatology, Venereology and
Leprosy and 2Psychiatry, RG Kar Medical College,
Kolkata, West Bengal, India.
Email:
abheek.sil@gmail.com
|
|
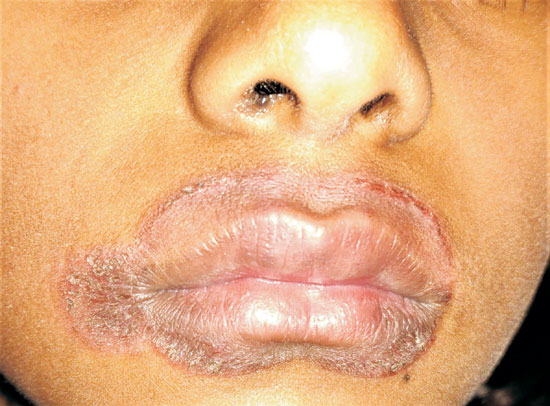
A 10-year-old girl presented with mildly pruritic
scaly rash around the lips for the past one month. She denied the use of
any lipstick, dentrifices or mouthwashes. On examination, there was a
well-demarcated erythematous plaque with scaling and fissuring,
symmetrically lining the perioral skin and vermilion margin of both lips
(Fig. 1). Rest of the mucocutaneous and systemic
examination was unremarkable. On further enquiry, her mother recalled
her ward’s recent habit of constantly licking the lips with the tongue.
A diagnosis of lip smacker’s cheilitis was made; topical fluticasone
cream and petrolatum jelly was prescribed.
 |
|
Fig. 1 Perioral erythema with
scale-crusts and fissures.
|
Lip smacker’s cheilitis is characterized by
persistent lip-licking, causing chronic inflammation of the vermilion
borders with clearly demarcated perioral erythema. Cheilitis may also
occur secondary to atopic dermatitis (presence of atopic stigmata),
psoriasis (scaly, erythematous plaque which elicits Grattage test and
Auspitz sign), long-term actinic exposure (lower lip affected commonly),
drugs (retinoids), and allergic contact (toothpaste, lipstick).
Behavioral therapy and topical tacrolimus, pimecrolimus cream, or
low-potent corticosteroid preparations are usually helpful.
|
|
|
 |
|
