|
|
|
Indian Pediatr 2017;54: 1005-1011 |
 |
Reference Centile Curves for Body Fat
Percentage, Fat-free Mass, Muscle Mass and Bone Mass Measured by
Bioelectrical Impedance in Asian Indian Children and Adolescents
|
|
Shashi Chiplonkar, Neha Kajale, Veena Ekbote, Rubina
Mandlik, Lavanya Parthasarathy,
*Ashwin Borade,
#Pinal Patel ,
#Prerna Patel, Vaman
Khadilkar and Anuradha Khadilkar
From Departments of Pediatrics, Hirabai Cowasji
Jehangir Medical Research Institute, Jehangir Hospital, Pune,
Maharashtra and *Inamdar Hospitals, Pune, Maharashtra; and #Department
of Biotechnology, Hemchandracharya North Gujarat University, Patan,
Gujarat, India.
Correspondence to: Dr Anuradha Khadilkar, Deputy
Director, Hirabai Cowasji Jehangir Medical Research Institute,
Jehangir Hospital, 32, Sassoon Road, Pune, Maharashtra, 411 001, India.
Email:
[email protected]
Received: June 07, 2016;
Initial review: January 10, 2017;
Accepted: August 21, 2017.
Published online:
September 26, 2017.
PII:S097475591600091
|
|
Objectives: To create
gender-specific percentile curves for percent body fat (%BF) by Bio
electrical Impedance Analysis (BIA) for screening adiposity and risk of
hypertension in Indian children and generate reference curves for
percent fat-free mass (%FFM), muscle mass (%LM) and bone mineral content
(BMC) by using bioelectrical impedance.
Design: Secondary analysis of
data from previous multicenter cross-sectional studies.
Setting: Private schools from
five regions of India.
Participants: A random sample of
3850 healthy school children (2067 boys) (5-17 yr) from private schools
in five major Indian cities.
Methods: Anthropometry, blood
pressure (BP) and body composition were measured by bioelectrical
impedance. Reference curves were generated by the LMS method.
Main outcome measures: %BF, %FFM,
%LM, BMC and BP
Results: Median %BF increased by
6% from 5 to 13 years of age and declined (around 2%) up to 17 years in
boys. In girls, %BF increased by 8% from 5 to 14 years and thereafter
declined by 3%. Based upon the risk of hypertension, the new cut-offs of
75th and 85th percentile of %BF were proposed for detecting over fatness
and excess fatness in children. Median %FFM was 90% at 5 yrs and
decreased till 12 years, and then showed a slight increase to 84% at 17
yrs in boys. In girls, it was 86% at 5 yrs and decreased till 15 yrs,
and plateaued at 71.8% at 17 yrs.
Conclusions: Reference curves for
percent body fat for Indian children would be useful to screen children
for health risk in clinical set up.
Key words: Body composition, Cut-offs,
Metabolic syndrome, Reference curves.
|
|
O
besity has become a major health concern in
childhood as it is a marker of cardio-metabolic risk in later life.
Recent studies have also demonstrated that not only excess fat mass [1]
but lean mass and muscle fitness [2] are also associated with health
risk. Assessment of body composition is an appropriate method to judge
adiposity and lean mass, and can help in early detection of cardio
metabolic risk.
Bioelectrical impedance (BIA) is a valuable
alternative to dual energy X-ray absorptiometry (DXA) in
assessing body composition as it is portable and convenient to use in
clinical setting and field surveys. However, a local reference database
is essential to assess the body composition status of children [3]. For
the DXA, we have generated such a reference database for Indian children
and adolescents [4-6]. However, lack of Indian reference values for BIA
reduces its utility to evaluate nutritional status, and associated
health risk in Indian children.
Thus, the objectives of the present study were: (i)
to create gender-specific percentile curves for percent body fat (%BF)
by BIA for screening adiposity in Indian children, (ii) to
explore the possible cut-offs of reference curves for risk of
hypertension, and (iii) to generate reference curves for percent
fat free mass (%FFM), muscle mass (%LM) and bone mineral content (BMC)
by BIA.
Methods
Data of 3832 schoolchildren (2054 boys) aged 5-17
years collected in previous cross-sectional studies were analyzed to
generate age- and gender-specific reference percentile curves for total
body fat percentage by BIA. It was a multicenter study conducted in 5
major cities (Delhi, Chennai, Pune, Kolkata and Raipur) from 5 states of
India [7] along with one center in Gujarat (Ahmadabad) during 2011 to
2014. Detailed methodology has been previously described [7]. From a
list of schools catering to children of socio-economically well-off
families from each city, six schools were randomly selected and
approached for permission to carry out measurements. All 2- to
17-year-old children from participating schools whose parents consented
to measurements were included [7]. The studies were approved by the
Ethics Committee of the Jehangir Clinical Development Pvt. Ltd., Pune,
which is a recognised Institute by Department of Scientific and
Industrial research (DSIR), Government of India.
Data were collected by the same team at each site;
equipments were calibrated daily. The mean inter- and intra-observer
coefficients of variation were <1% for weight, height and body
composition measurements.
Height-for-age (HAZ), weight-for-age (WAZ) and
BMI-for-age (BAZ) Z-scores were computed as deviations from the
median [8]. Adult equivalent BMI Z scores were also computed
using adult equivalent values for Asians [9] as normal weight (BMI at
age 18 d-23 kg/m 2),
overweight (BMI 23 to 28 kg/m2)
and obese (BMI >28 kg/m2).
Body composition was assessed using Bioelectrical
Impedance Analyzer (BIA), (Tanita Model BC-420MA) after a minimum of 3
hours of fasting, and voiding before measurements (10 am onwards) [10].
This analyzer measures body composition using a constant current source
with a high frequency current (50kHz, 90µA). The 8 electrodes are
positioned so that electric current is supplied from the electrodes on
the tips of the toes of both feet, and voltage is measured on the heel
of both feet. BIA measures body composition as fat%, fat mass, fat free
mass, total body water, bone-free lean tissue mass (LTM), bone mineral
amount included in the entire bone (bone mass) by measuring
bioelectrical impedance in the body in standing position of subject.
Measurements were tested for test-retest reliability on pilot sample of
ten subjects separately by measuring them on BIA at two different time
points. Reliability coefficient was significant for the body fat
percent, fat mass, fat-free mass and muscle mass (intra class
correlation coefficient = 0.96, P=0.0001). Clinical examinations
were carried out by pediatricians to assess health status of children to
ensure that only apparently healthy children were included in the study.
Statistical analysis: All statistical analyses
were performed using SPSS software (version 16.0. 2007). All results
were expressed as mean (SD) for comparability with other studies.
Smoothed gender-specific reference plots showing 2nd, 9th, 25th, 50th,
75th, 85th and 95th percentiles of %BF and FFM were derived using LMS
method (LMS chart-maker Pro version 2.4, 2008; by Pan and Cole), which
constructs reference percentiles adjusted for skewness [11]. Each
variable of interest was summarized by three smooth curves plotted
against age, representing the median (M), coefficient of variation (S)
and skewness (L) of the measurement distribution [12]. Models were
checked for goodness of fit using the detrended Q-Q plot, Q Tests and
worm plots [13]. The LMS method was found to be appropriate to use for
this data as the measure of skewness of the data was 1.1 with a standard
error of 0.03. The possible cut-offs of derived %BF percentiles were
tested for their efficacy against the BP values by classifying the
children into three groups: normal BP (SBP/DBP <90th percentile),
pre-hypertension (SBP/DBP 90th-95th percentile), and hypertension
(SBP/DBP >95 th percentile)
[14]. Pearson’s correlation coefficient was used to assess relationship
of BP and various body composition parameters, i.e. BMI, FMI,
LMI, FFMI and %BF.
Results
Table I illustrates anthropometric and body
composition parameters for both the genders from 5 to 17 years of age.
Mean (SD) height-for-age Z-scores in boys [girls] were 0.11 (1.0) [0.10
(1.0)]; weight for age Z-scores were 0.25 (1.0) [0.12 (1.1)] and BMI for
age Z-scores were 0.21 (0.98) [0.09 (1.1)]. Majority of the children
(95.5%) had normal Z-scores for height, weight and BMI with reference to
contemporary Indian growth references [8].
TABLE I Anthropometry and Body Composition Measurements by Age and r in Indian Children and Adolescents
|
Age (yr) |
n |
Height (cm) |
Weight (kg) |
Fat Mass (kg) |
Fat-free mass |
Muscle mass |
Bone mineral |
Fat Percent
|
|
|
|
|
|
(kg) |
(kg) |
content (kg) |
|
|
Boys |
|
5 |
36 |
114.6 (5.2) |
20.5 (5.1) |
2.9 (3.2) |
17.5 (2.2) |
16.8 (2.0) |
0.7 (0.2) |
12.2 (8.1) |
|
6 |
145 |
118.6 (5.7) |
22.3 (4.7) |
3.6 (3.2) |
18.9 (2.2) |
18.1 (2.1) |
0.8 (0.1) |
14.3 (8.7) |
|
7 |
120 |
124.5 (5.5) |
25.2 (5.4) |
4.4 (4.1) |
21.0 (2.3) |
20.1 (2.2) |
0.9 (0.1) |
15.5 (10.5) |
|
8 |
144 |
129.0 (6.4) |
27.4 (5.4) |
4.6 (4.7) |
22.8 (2.6) |
21.7 (2.5) |
1.0 (0.2) |
14.7 (10.4) |
|
9 |
177 |
135.4 (6.7) |
32.3 (7.6) |
6.7 (5.8) |
25.5 (2.9) |
24.3 (2.7) |
1.2 (0.2) |
18.4 (11.3) |
|
10 |
176 |
140.7 (7.0) |
36.4 (8.4) |
8.4 (6.7) |
28.0 (3.4) |
26.6 (3.2) |
1.4 (0.2) |
20.5 (12.3) |
|
11 |
232 |
145.8 (8.2) |
40.2 (11.7) |
9.2 (9.4) |
30.8 (4.1) |
29.2 (3.9) |
1.5 (0.2) |
19.8 (12.7) |
|
12 |
268 |
151.4 (8.0) |
44.1 (11.6) |
10.2 (9.3) |
34.3 (4.9) |
32.6 (4.6) |
1.7 (0.3) |
19.9 (12.8) |
|
13 |
234 |
156.9 (8.5) |
48.1 (11.2) |
10.4 (8.9) |
37.8 (5.5) |
35.9 (5.2) |
2.0 (0.3) |
19.9 (11.9) |
|
14 |
175 |
164.4 (7.5) |
56.2 (13.0) |
13.2 (10.8) |
43.3 (5.3) |
41.0 (5.0) |
2.3 (0.3) |
20.9 (12.3) |
|
15 |
146 |
167.7 (6.8) |
58.4 (13.4) |
11.5 (9.4) |
47.2 (6.1) |
44.7 (5.7) |
2.5 (0.3) |
17.5 (10.5) |
|
16 |
131 |
169.2 (6.7) |
60.1 (12.2) |
10.2 (6.9) |
50.5 (7.1) |
47.8 (6.8) |
2.6 (0.3) |
15.7 (7.5) |
|
17 |
70 |
170.3 (6.4) |
63.8 (12.8) |
11.6 (7.5) |
52.5 (6.8) |
49.8 (6.7) |
2.7 (0.3) |
16.9 (7.6) |
|
Girls |
|
5 |
40 |
114.1 (5.6) |
20.3 (4.0) |
3.3 (2.2) |
16.8 (2.2) |
16.0 (2.1) |
0.7 (0.1) |
15.4 (6.7) |
|
6 |
126 |
117.6 (5.8) |
21.7 (5.3) |
3.7 (2.7) |
17.9 (2.8) |
17.09 (2.6) |
0.8 (0.1) |
15.5 (7.3) |
|
7 |
95 |
123.8 (5.9) |
24.5 (5.6) |
4.6 (3.4) |
19.9 (2.6) |
19.0 (2.4) |
0.9 (0.2) |
17.2 (8.2) |
|
8 |
135 |
129.6 (6.6) |
28.5 (8.2) |
6.2 (4.9) |
22.4 (3.8) |
21.3 (3.5) |
1.1 (0.3) |
19.3 (9.1) |
|
9 |
122 |
133.8 (6.7) |
30.7 (8.1) |
6.6 (5) |
23.9 (3.9) |
22.7 (3.6) |
1.23 (0.3) |
19.3 (9.4) |
|
10 |
181 |
139.6 (8.0) |
33.9 (9.0) |
7.7 (5.3) |
26.3 (4.6) |
24.9 (4.2) |
1.4 (0.3) |
20.4 (9.2) |
|
11 |
205 |
146.6 (7.7) |
38.5 (9.6) |
8.9 (5.8) |
29.6 (4.9) |
27.9 (4.5) |
1.7 (0.4) |
21.1 (9.0) |
|
12 |
244 |
150.1(7.0) |
41.8 (9.7) |
10.4 (6.3) |
31.5 (4.4) |
29.7 (4.1) |
1.8 (0.3) |
23.2 (8.9) |
|
13 |
215 |
153.8 (6.7) |
46.7 (10.8) |
13.1 (7.3) |
33.7 (4.6) |
31.7 (4.2) |
2 (0.3) |
26.0 (9.2) |
|
14 |
147 |
155.4 (6.0) |
50.7 (10.9) |
16.1 (8.5) |
34.6 (4.1) |
32.6 (3.8) |
2.0 (0.3) |
30.1 (8.1) |
|
15 |
117 |
156.6 (5.6) |
52.3 (9.1) |
16.1 (6.7) |
36.2 (3.7) |
34.1 (3.4) |
2.1 (0.3) |
29.8 (6.8) |
|
16 |
103 |
157.0 (6.1) |
51.1 (8.3) |
14.6 (5.1) |
36.5 (4.1) |
34.5 (3.8) |
2.0 (0.4) |
27.8 (5.7) |
|
17 |
48 |
158.4 (7.4) |
55.1 (11.6) |
16.5 (7.6) |
38.7 (6.1) |
36.5 (5.7) |
2.2 (0.4) |
28.9 (6.6) |
|
Values are Mean (SD). |
When compared with adult-equivalent cut-offs of BMI
for Asians corresponding to 23 and 28 kg/m 2
[9], 65.2% boys (86.9% girls) had normal BMI, 23.3% boys (11.1% girls)
had BMI >23 kg/m2 adult
cut-off and 11.5% boys (2% girls) had >28 kg/m2
adult cut-off.
Mean body fat percent in boys and girls increased
gradually till 14 years of age and then showed a decline up to 17 years;
though the decline was small and mean fat percent was higher in girls
than boys (P<0.05). Mean muscle mass and fat-free mass also
increased with age in both boys and girls though boys had a
significantly higher muscle mass than girls after 11 years of age (P<0.05).
Bone mass of boys and girls increased with age, and after 13 years of
age, bone mass of girls showed a plateau while boys showed increase till
17 years.
BMI showed a significant correlation with %BF
(r=0.87, P <0.01). Considering the adult equivalent Asian BMI
cut-offs of obesity and adiposity, 90.8% of boys and 91.8% of girls with
high adiposity were correctly identified by BMI (sensitivity or
true-positive rate), and 91.7% of boys and 82.2% of girls without high
adiposity were also correctly classified (specificity or true-negative
rate). Among those adolescents considered as overweight or obese by BMI
cut-offs, only 69.3% of girls and 85.0% of boys had excess adiposity
(the predictive value).
With advancing age, SBP and DBP increased slowly; the
mean blood pressure was within reference range [14] in 87% boys and 90%
girls. BMI showed a significant correlation with SBP (r= 0.67, P<0.01)
and DBP (r= 0.54, P<0.01). A positive significant correlation was
observed between percent body fat with SBP (r=0.53, P<0.01) and
DBP (r=0.44, P<0.01). According to hypertension cut-offs, 41.1%
overweight or obese boys and 30.6% girls showed high blood pressure,
whereas with excess fatness 45% boys and 36.4% girls were having
hypertension. Around 4% to 6% children and adolescents were
misclassified as hypertensive with BMI cut-offs than the BIA cut-offs as
also with the proposed body fatness cut-offs.
To examine the relative fatness with height, indices
of fat mass, muscle mass and body mass were computed (Table II).
In boys with increasing age, average increase in FMI and BMI was around
3% whereas increase in Muscle mass index (MMI ) was 7%. In girls, BMI
showed a similar rate of increase of 3% with age but average increase in
FMI was 9% and in MMI 1.4%. The correlations of SBP with FMI, MMI, and
BMI (r=0.57-0.69, P<0.01) even after adjusting for age in both
boys and girls.
TABLE II Fat Mass Index, Muscle Mass Index and Body Mass Index by Age in Boys and Girls
|
Age (yr) |
Boys |
|
|
|
Girls |
|
|
|
|
FMI
|
MMI
|
FFMI
|
BMI
|
FMI
|
MMI |
FFMI
|
BMI |
|
5 |
2.06 (2.0) |
12.56 (0.7) |
13.26 (0.7) |
15.41 (2.6) |
2.50 (1.5) |
12.26 (0.8) |
12.82 (0.9) |
15.52 (2.2) |
|
6 |
2.45 (2.0) |
12.79 (0.5) |
13.36 (0.6) |
15.76 (2.3) |
2.56 (1.7) |
12.27 (0.9) |
12.87 (1.0) |
15.50 (2.6) |
|
7 |
2.81 (1.8) |
12.80 (0.6) |
13.51 (0.5) |
16.15 (2.8) |
2.90 (2.0) |
12.30 (0.8) |
12.94 (0.9) |
15.84 (2.8) |
|
8 |
2.67 (2.5) |
12.91(0.7) |
13.65 (0.7) |
16.3 4(2.8) |
3.55 (2.5) |
12.62 (1.1) |
13.28 (1.2) |
16.73 (3.5) |
|
9 |
3.56 (2.9) |
13.22 (0.6) |
13.87 (0.5) |
17.49 (3.0) |
3.56 (2.5) |
12.59 (1.0) |
13.27 (1.1) |
16.89 (3.4) |
|
10 |
4.13 (3.2) |
13.41 (0.7) |
14.08 (0.7) |
18.21 (3.2) |
3.79 (2.5) |
12.87 (1.0) |
13.61 (1.1) |
17.19 (3.3) |
|
11 |
4.27 (3.8) |
13.74 (0.8) |
14.54 (0.8) |
18.71 (3.9) |
4.06 (2.6) |
13.04 (1.2) |
13.72 (1.3) |
17.74 (3.6) |
|
12 |
4.21 (3.9) |
14.07 (0.9) |
14.84 (0.9) |
19.04 (4.1) |
4.57 (2.8) |
13.40 (1.0) |
14.22 (1.1) |
18.42 (3.5) |
|
13 |
4.17 (3.7) |
14.45 (0.9) |
15.37 (0.9) |
19.48 (3.8) |
5.42 (2.9) |
13.54 (1.1) |
14.38 (1.2) |
19.62 (3.7) |
|
14 |
4.74 (3.9) |
15.05 (1.0) |
16.0 (1.0) |
20.58 (4.3) |
6.67 (3.5) |
13.47 (1.1) |
14.41(1.3) |
21.02 (4.1) |
|
15 |
4.11 (3.4) |
15.86 (1.4) |
16.75 (1.5) |
20.72 (4.6) |
6.57 (2.6) |
13.88 (1.0) |
14.72 (1.0) |
21.31 (3.3) |
|
16 |
3.58 (2.4) |
16.65 (2.0) |
17.58 (2.0) |
20.95 (3.9) |
5.94 (2.1) |
13.98 (1.1) |
14.81 (1.2) |
20.74 (3.1) |
|
17 |
3.85 (2.5) |
16.95 (1.7) |
18.0 (1.8) |
22.01 (4.1) |
6.57 (2.6) |
14.50 (1.6) |
15.37 (1.7) |
21.91 (4.0) |
|
*Values are Mean ± SD; FMI = Fat Mass Index (Fat mass (kg)/
Height2 (m)); MMI = Muscle Mass Index (Muscle Mass
(kg)/Height2 (m); FFMI = Fat Free Mass Index (Fat
Free Mass (kg)/ Height2 (m)); BMI = Body Mass Index
(weight (kg)/Height2 (m)). |
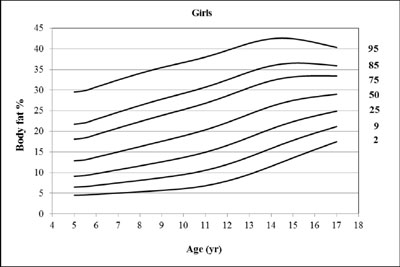
The reference percentile curves generated for %BF by
BIA are illustrated in Fig. 1a (boys) and Fig.
1b (girls). A significant gender difference was seen in the shape of
fat percentile curves. Lower percentiles of boys were flatter than girls
and around 10 years of age, body fat% showed higher increase in girls
than boys. Median fat% percentile of boys was also lower than the median
percentile of girls. Median fat% of boys declined after 13 years of age
while for girls there was a steady increase with age. Median fat percent
in boys showed an average increase of 6% from 5 to 13 years of age, and
then a decline of around 2% up to 17 years of age. However, median fat%
in girls increased by 8% from 5 to 14 yrs, and by 3% thereafter up to 17
years of age.

(a) |
(b) |
|
Fig.1 Smoothed reference percentile
curves for percent body fat for Indian boys (a); and girls (b).
|
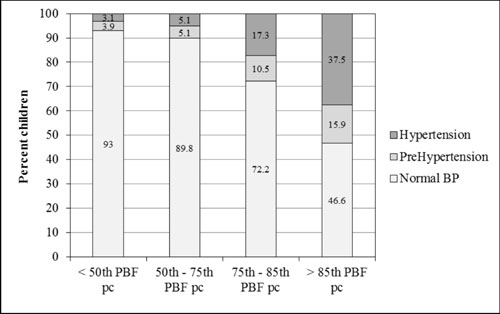
To explore the association of over fatness and
obesity with the risk of hypertension, the percentages of children in
the hypertensive or pre-hypertensive range or with BP <90th percentile
wereclassified in successive fat percentile categories. It was observed
that %BF percentile groups; with <50th, 50th-75th, 75th-85th, and >85th
reference percentile, exhibited a significant
difference in prevalence of hypertension in various percentile groups (P<0.01).
Up to the 75th fat percentile, the percent children with hypertension
was relatively small which increased in the later %BF percentile groups
(P<0.05). Percentage of children with pre-hypertension also
increased from the 75th percentile (P<0.05). Thus, the75th and
85th reference percentiles may reveal the risk of hypertension (Fig.
2).
 |
|
Fig. 2 Association of hypertension
risk with degree of fatness by Indian body fat percentiles.
|
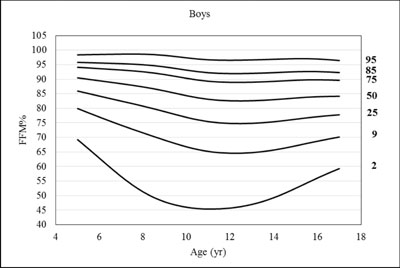
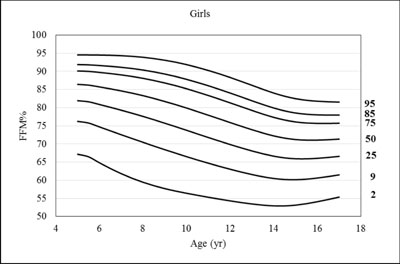
Reference percentiles for %FFM by age and gender are
provided in Fig. 3a and 3b, respectively.
Median percentile of %FFM was 90% at 5 years of age, and it decreased
gradually to 82.5% by 12 years of age in boys, after which it increased
gradually to 84% at the age of 17 years. In girls, the 50th percentile
of %FFM was lower (86% at 5 yr of age) than boys and it decreased to 71%
by 15 years of age and showed a plateau till 17 years of age.
(a) |
(b) |
|
Fig. 3 Smoothed Reference
percentile curves for percent FFM for Indian boys (a); and girls
(b).
|
WebFig. 1a
and 1b
represent reference curves for percent muscle mass in boys and girls,
respectively. In boys, the lower percentiles (2nd and 9th) exhibit a dip
between 7 to 14 years of age and then show a small increase till 17
years; while, higher percentiles are flat and almost parallel to the
horizontal axis. In girls, average decrease of 0.8% was seen in median
%lean mass with increasing age.
Reference curves for bone mineral content by BIA for
Indian boys and girls showed increasing trend with age till 17 year in
boys (Web Fig. 2a) and till 15 year in girls (Web
Fig. 2b). In boys, 50th percentile of BMC increased
rapidly up to 13 year and then gradually till 17 year of age. In girls,
median percentile of BMC showed an increase up to 11 year of age after
which the curve was flatter till 17 year of age.
Discussion
The present study describes age-and gender-specific
reference curves for body fat percentage measured by BIA (BC-420MA) for
children and adolescents using a large sample representing various
regions of India. The possible cut-offs of 75th and 85th percentile have
been suggested based on the risk of hypertension for defining over fat
and excess fat, respectively. Our study also provides reference
percentiles of %FFM, %LM and BMC by age and gender.
The present fat mass percentiles are device- and
country-specific, and may not be applicable to other BIA devices.
Another limitation of the study is that the cut-offs for %BF and various
body composition parameters could not be assessed with metabolic
markers. Unlike what is known about BMI and Waist circumference [15],
there are no meaningful cut-off values established to indicate
cardiovascular and metabolic risk. We used hypertension as a marker for
health risk and proposed the ‘excess fat’ cut-offs. Our results showed a
better correlation of BMI with blood pressure than %BF. This may be due
to use of adult equivalent Asian BMI cut-offs over IOTF or other
cut-offs. However, misclassification of hypertension risk was more with
BMI cut-offs than proposed excess fatness cut-offs. These results
suggest the utility of body fat assessment in evaluating possible health
risk in youth. Results also indicate the need for future research to
establish Indian population-specific prediction equations for BIA
estimates of total body water and fat mass.
When compared with other BIA fat percentile data,
median fat percentage of Indian boys was lower than the UK, Turkish,
German and Chinese boys till the age of 12 years, and then it overlapped
with the UK and Turkish boys but remained lower than that of Chinese and
German boys [16-19] (Web Fig. 3a). Indian and
Chinese girls’ median fat percentage was similar with both showing a
steady rise with age. Till the age of 13 years, Indian and Chinese
median curves were lower than UK, German and Turkish girls and were
higher thereafter (Web Fig. 3b). The 85th and 95th %BF
percentiles of Indian boys and girls were higher than that of the UK,
German and Turkish children (Web Fig. 3c and 3d).
Thus, the shape of the Indian fat percentile curves was different,
especially during pubertal years, than the UK standards and other
population based studies. Therefore, these western reference standards
may not assess fatness uniformly over the entire childhood age-range for
children of Asian Indian origin. Though some part of these variations
may be attributable to the differences in the model and make of BIA
instruments [19], the reference curves derived in this study from Indian
data may be more appropriate for assessing fatness in Asian Indian
children and adolescents.
Percentiles for fat free mass by BIA in adults have
been reported [20]. Though %FFM percentiles in pediatric age range have
been recently reported in UK population [21], such data are not
available for Asian populations. The 50th percentile of UK boys was flat
across the age range which is in agreement with our data. For UK girls,
the 50th percentile of %FFM was lower compared with boys and declined
with age until around 11 years of age (the mean age at which puberty
commences); it then continued to decrease at a slower rate up to age 17
years. Indian girls in the present study also showed a similar decline
in % FFM with age; however, the age of decline and magnitude of %FFM are
lower in our data than in the UK girls and boys.
In summary, suggested reference curves for percent
body fat, fat free mass, muscle mass and bone mineral content by BIA for
Asian Indian children may be useful to assess body composition in
children in clinical and community set up. A cut off of 75th
and 85th percentile of %BF
may further be beneficial to detect over fatness and excess fatness in
Asian Indian children.
Acknowledgments: Director, HCJMRI, Dr. Uma Divate
for giving us permission for carrying out this study.
Contributors: SAC, AVK, VVK, VHE and NAK designed
research; SAC, AVK, VVK, VHE, NAK, LP, RM, AB, PP and PP conducted
research; SAC, AVK, VHE, NAK and RM analyzed data; SAC, AVK, VHE, NAK
and VVK wrote the paper; AVK had primary responsibility for final
content. All authors read and approved the final manuscript.
Funding: Novo Nordisk India Pvt. Ltd.
Competing interest: None stated.
|
What is Already Known?
• Body fat percentage for a given BMI is
higher in Asian Indian children in comparison to their Caucasian
counterparts.
What This Study Adds?
• Reference centile curves for body fat
percentage, fat-free mass and muscle mass for Asian Indian
children and adolescents are provided.
• Based on the risk of hypertension, cut offs
of 75th and 85th percentile of body fat percentage have been
suggested for correctly classifying excess fatness in clinical
and community settings.
|
References
1. Jahagirdar R, Hemchand KP, Chiplonkar SA,
Khadilkar VV, Khadilkar AV. Relationship between body mass index, fat
distribution and cardio-metabolic risk factors in Indian children and
adolescents. Pediatr Obes. 2012;7:E37-41.
2. Weber DR, Leonard MB, Shults J, Zemel BS. A
comparison of fat and muscle body mass index to BMI for the
identification of metabolic syndrome in children and adolescents. J Clin
Endocrinol Metab. 2014;99:3208-16.
3. Pandit D, Chiplonkar S, Khadilkar A, Khadilkar V,
Ekbote V. Body fat percentages by dual-energy X-ray
absorptiometry corresponding to body mass index cutoffs for overweight
and obesity in Indian children. Clin Med Pediatr. 2009;3:55-61.
4. Khadilkar AV, Sanwalka NJ, Chiplonkar SA,
Khadilkar VV, Pandit D. Body fat reference percentiles on healthy
affluent Indian children and adolescents to screen for adiposity. Int J
Obes (Lond). 2013;37:947-53.
5. Jebb S, McCarthy D, Fry T, Prenice AM. New body
fat reference curves for children. Obesity Reviews ( NAASO supple.)
2004;A 156. Available from: http://media.tanita.com/data/Children’s_Body_Fat_Chart_
OTHERS_others_OTHERS__011b.jpg?rev=E5A0. Accessed June 01, 2016.
6. Liu A, Byrne NM, Kagawa M, Ma G, Kijboonchoo K,
Nasreddine L, et al. Ethnic differences in body fat distribution
among Asian pre-pubertal children: A cross-sectional multicenter study.
BMC Public Health. 2011;11:500.
7. Khadilkar A, Ekbote V, Chiplonkar S, Khadilkar V,
Kajale N, Kulkarni S, et al. Waist circumference percentiles in
2-18 year old Indian children. J Pediatr. 2014;164:1358-62.
8. Indian Academy of Pediatrics Growth Charts
Committee, Khadilkar V, Yadav S, Agrawal KK, Tamboli S, Banerjee M
Cherian A, et al. Revised IAP Growth charts for height, weight
and body mass index for 5- to 18-year-old Indian Children. Indian
Pediatr. 2015;52:47-55,
9. Khadilkar VV, Khadilkar AV, Borade AB, Chiplonkar
SA. Body mass index cut-offs for screening for childhood overweight and
obesity in Indian children. Indian Pediatr. 2012;49:29-34.
10. Kyle UG, Bosaeus I, De Lorenzo AD, Deurenberg P,
Elia M, Manuel Gómez J, et al. Bioelectrical impedance
analysis-part II: Utilization in clinical practice. Clin Nutr.
2004;23:1430-53.
11. van ‘t Hof MA, Wit JM, Roede MJ. A method to
construct age references for skewed skinfold data, using Box-Cox
transformations to normality. Hum Biol. 1985;57:131-9.
12. Cole TJ, Green PJ. Smoothing reference centile
curves: the LMS method and penalized likelihood. Stat Med. 1992;11:
1305-19.
13. van Buuren S, Fredriks M. Worm plot: A simple
diagnostic device for modelling growth reference curves. Stat Med.
2001;20:1259-77.
14. Raj M, Sundaram R, Paul M, Kumar K. Blood
Pressure distribution in Indian children. Indian Pediatr. 2010;47:
477-85.
15. Sung RY, Yu CC, Choi KC, McManus A, Li AM, Xu SL,
et al. Waist circumference and body mass index in Chinese children:
cutoff values for predicting cardiovascular risk factors. Int J Obes (Lond).
2007;31:550-8.
16. McCarthy HD, Cole TJ, Fry T, Jebb SA, Prentice
AM. Body fat reference curves for children. Int J Obes. 2006;30:598-602.
17. Kurtoglu S, Mazicioglu MM, Ozturk A, Hatipoglu N,
Cicek B, Ustunbas HB. Body fat reference curves for healthy Turkish
children and adolescents. Eur J Pediatr. 2010;169:1329-35.
18. Plachta-Danielzik S, Gehrke MI, Kehden B,
Kromeyer-Hauschild K, Grillenberger M, Willhöft C, et al. Body
fat percentiles for German children and adolescents. Obes Facts.
2012;5:77-90.
19. Sung RY, So HK, Choi KC, Li AM, Yin J, Nelson EA.
Body fat measured by bioelectrical impedance in Hong Kong Chinese
children. Hong Kong Med J. 2009;15:110-17.
20. Pichard C, Kyle UG, Bracco D, Slosman DO, Morabia
A, Schutz Y. Reference values of fat-free and fat masses by
bioelectrical impedance analysis in 3393 healthy subjects. Nutrition.
2000;16:245-54.
21. McCarthy HD, Samani-Radia D, Jebb SA, Prentice
AM. Skeletal muscle mass reference curves for children and adolescents.
Pediatr Obes. 2014;9:249-59.
|
|
|
 |
|
