|
|
|
Indian Pediatr 2016;53: 1103-1105 |
 |
Infantile Intraosseous
Maxillary Hemangioma
|
|
Divya Gupta, Ishwar Singh, Kavita Goyal and
*Parul Sobti
From Departments of Otorhinolaryngology and Head and
Neck Surgery, and *Pathology, Maulana Azad Medical College and
associated Lok Nayak Hospital, New Delhi, India.
Correspondence to: Dr Divya Gupta, Department of
Otolaryngology and Head & Neck Surgery, Maulana Azad Medical College and
associated Lok Nayak Hospital, New Delhi, India.
Email:
[email protected]
Received: October 09, 2015;
Initial review: October 28, 2015;
Accepted: August 06, 2016.
|
Background: Primary osseous hemangiomas of the facial skeleton mimic
malignancy. Their location in maxillary sinus, especially in infants is
extremely rare. Case character-istics: 1- month-old full term boy
with maxillary swelling. Observations: Biopsy from oral route
revealed hemangioma showing vascular channels lined by endothelial
cells. Patient improved on oral steroids. Message: Hemangiomas
should be considered as one of the differential diagnosis of unilateral
maxillary swelling in infants. Steroids may serve as the primary mode of
treatment as opposed to tumor excision.
Keywords: Corticosteroids, Maxilla, Tumor, Vascular
malformations.
|
|
H
emangiomas are benign tumors of the capillary
endothelium, and have varied clinical presentations. Intraosseous
hemangioma is a rare tumor accounting for 0.2-0.7% of all bone tumors
[1]. It is seen more frequently in vertebrae and calvarium, and is very
rare in jaw bones. Two-thirds of the jaw lesions occur in mandible and
one-third are found in maxilla [2]. Primary intraosseous maxillary
hemangioma in infants is extremely rare [3,4].
Case Report
A one-month-old male infant presented to us with
progressive right maxillary swelling and alveolar fullness, first noted
at 6 days of age. The child was born term, and had no significant
perinatal history. No functional deficits due to maxillary mass were
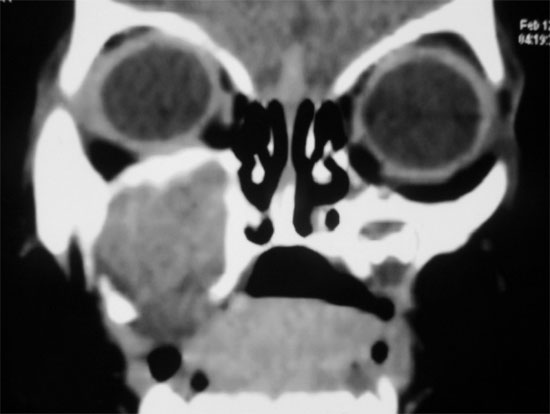
reported. Computed tomography (CT) revealed a heterogeneous, mildly
enhancing and expansile lesion of the right maxilla, replacing the right
maxillary sinus and alveolar ridge. Orbital contents were normal (Fig.
1).
 |
|
Fig. 1 CT scan showing mildly
enhancing expansile lesion of the right maxilla.
|
We suspected malignancy, and performed a biopsy from
the swelling under general anesthesia via sublabial route. A fleshy
bleeding mass was seen from which biopsy was taken. The mass bled
profusely and the maxillary sinus was packed with sofragauze. The pack
was subsequently removed gently under short inhalational anesthesia
after two days. No bleeding was seen subsequently. Histopathological
examination of the mass revealed hemangioma showing vascular channels
lined by increased number of bland endothelial cells with no atypia or
mitosis. We treated the child with oral steroids (2 mg/kg/day) for two
months followed by gradual fortnightly tapering after the lesion
regressed. Maxillary fullness resolved in four months. The patient is
now well on regular follow-up.
Discussion
Infantile hemangiomas appear in infancy, grow till
one year of age, are more in females, and involute by adolescence. They
usually do not involve the bone, and are histologically characterized by
endothelial hyperplasia and increased number of mast cells with
expression of glucose transporter-1 (GLUT-1). Congenital hemangiomas;
however, have no postnatal proliferative phase [5]. This distinct
behaviour disqualifies the possibility of congenital hemangioma in this
child, as the maxillary swelling gradually increased in size. On the
other hand, vascular malformations are present at birth, have equal
gender distribution and usually become more prominent by puberty because
of slow progressive ectasia resulting from intraluminal flow. They do
not show endothelial hyperplasia and have normal number of mast cells
[4]. Venous malformations are very commonly mistaken to be hemangiomas.
It was easy to confuse hemangioma with vascular malformations in this
case as the presentation was congenital. We could not check GLUT-1
expression in this case because of unavailability of the marker kit but
the increased number of endothelial cells on histology, relatively rapid
increase in swelling size, and reversal of maxillary fullness on
treatment with steroids pointed strongly towards this lesion being a
hemangioma.
Intraosseous hemangiomas have a variable presentation
and occur mostly in second decade of life with a 2:1 preponderance in
females [6]. Incidentally, the two earlier reported cases of infantile
intraosseous maxillary hemangioma were both females [3,4].
CT of such lesions may show homogenous, non-calcified
masses that may remodel adjacent bone and show enhancement on contrast
administration [7]. It may also cause bony destruction leading to a
false impression of malignancy. Confirmation of the diagnosis requires
biopsy, but that is likely to result in profuse bleeding as in our case.
Hence, a very small antral window needs to be created for taking biopsy
from maxilla through sublabial route so that bleeding could be minimized
by pressure packing.
The treatment options of intraosseous hemangiomas
include complete excision of the tumor with reconstruction using various
materials. This may or may not be preceded by embolization [8]. However,
these recommendations have largely been made on the basis of treatment
of adult patients. Hemangiomas in infancy run growth phases of
progression and involution, and there is always a possibility of the
lesion resolving completely by itself with time. Moreover, any major
surgical manipulation in the bony framework of an infant may result in
permanent deformity. Keeping these points in consideration and with the
primary aim of arresting the growth of lesion and reducing the
likelihood of permanent disfigurement, we started treatment with oral
steroids, which resulted in a good response. Werle, et al. [3]
also reported complete resolution of maxillary hemangioma in an infant
girl with a ten-month course of oral steroids.
We suggest that possibility of hemangiomas should
always be considered in unilateral maxillary swelling in infants.
Conservative treatment with oral steroids may be the first line of
management in infantile intraosseous hemangiomas.
Contributors: DG and PS: case management and
drafting the manuscript; IS and KG: supervision of case and revision of
manuscript. All the authors approved the final version of the
manuscript.
Funding: None; Competing interests: None
stated.
References
1. Faeber T, Hiatt WR. Hemangioma of the frontal
bone. J Oral Maxillofac Surg. 1991;49:1018.
2. Mutlu M, Yaris N, Aslan Y, Kul S, Imamoglu M,
Ersoz S. Intraosseous noninvoluting congenital hemangioma of the
mandible in a neonate. Turkish J Pediatr. 2009;51:507-9.
3. Werle AH, Kirse DJ, Nopper AJ, Toboada EM. Osseous
hemangioma of the maxilla in an infant. Otolaryngol Head Neck Surg.
2003;128:906-9.
4. Kadlub N, Dainese L, Hermine ACL, Galmiche L,
Soupre V, Lepointe HD, et al. Intraosseous hemangioma: semantic
and medical confusion. Int J Oral Maxillofac Surg. 2015;44:718-24.
5. Darrow DH, Greene AK, Mancini AJ, Nopper AJ.
Diagnosis and management of infantile hemangioma. Pediatrics.
2015;136:e1060-104.
6. Jeter TS, Hackney FL, Aufdemorte TB. Cavernous
hemangioma of the zygoma: report of cases. J Oral Maxillofac Surg.
1990;48:508-12.
7. Koch BL, Myer CM. Presentation and diagnosis of
unilateral maxillary swelling in children. Am J Otolaryngol.
1999;20:106-29.
8. Yung YW, Sheng MG, Merrill RG, Sperry DW. Central Hemangioma of
the jaws. J Oral Maxillofac Surg. 1989;47:1154-60.
|
|
|
 |
|
