|
|
|
Indian Pediatr 2011;48: 9 68 |
 |
Bullous Congenital Ichthyosiform Erythroderma |
|
Ashim Kumar Mondal, Piyush Kumar and Avijit Mondal
Department of Dermatology, Medical College and Hospital,
88, College street, Kolkata 700 073, West Bengal.
Email: [email protected]
|
|
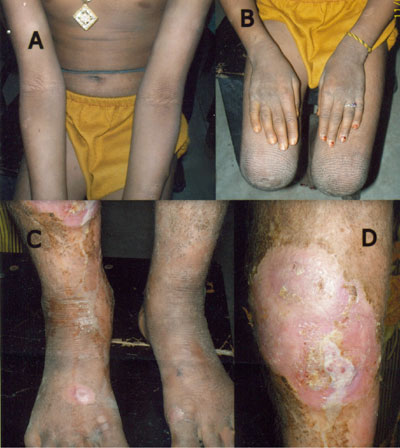
An 8 years-old girl presented with intermittent bullous lesions and rough
thick skin since birth. At birth, her skin was reddish in color and was
notable for spontaneous peeling. Soon after birth, she developed a bulla
over leg, which healed spontaneously in 2 weeks without any scarring or
pigmentation. However, she kept developing bullae intermittently. At
around 5 months of age, she developed gradual thickening of skin. On
examination, skin was dry and scaly. "Corrugated cardboard" like thickened
skin was noted around joints, involving both extensor and flexor surfaces.
Single erosion was found on right shin (Fig. 1). Systemic
examination was non-contributory. Based on clinical presentation, she was
diagnosed with bullous congenital ichthyosiform erythroderma (bullous CIE).
Histopathology from the erosion showed marked hyperkeratosis, a thick
granular layer, and vacuolar degeneration of the upper epidermis. These
findings were consistent with the diagnosis of bullous CIE.
 |
|
Fig. 1 Note "Corrugated cardboard" like
hyperkeratosis in popliteal fossa (A), wrist and knee (B), and
cubital fossa (C). Erosion over right shin (D). |
Bullous CIE is a rare autosomal dominant genodermatosis
caused by mutation in epidermal keratins 1 and 10. It presents as
erythroderma (involvement of more than 90% of skin with erythema, scaling
with/without edema) and blistering in newborns, followed by a lifelong
ichthyotic condition. As patients age, the scaling becomes thicker and the
propensity to blister decreases. Palms and soles may be involved. This
condition should be differentiated from non-bullous CIE (absence of
history of bullae, presence of erythroderma) and epidermolysis bullosa
(bulla formation at trauma prone areas, variable scarring absence of
scaling or hyperkeratosis). The diagnosis is usually clinical;
histopathology findings help in making a diagnosis. The term "epidermolytic
hyperkeratosis" is often used as synonym for bullous CIE. Treatment in
early period is directed towards treating secondary complications of
erosions (sepsis, electrolyte imbalance etc). Later in life, emollients,
urea 10%, topical and systemic retinoids are helpful.
|
|
|
 |
|
