|
|
|
Indian Pediatr 2009;46: 1102-1103 |
 |
Etiological Spectrum of Acute Intestinal
Obstruction |
|
Venkatesh M Annigeri, JK Mahajan and KLN Rao,
Department of Pediatric Surgery, Advanced Pediatrics
Centre,
PGIMER, Chandigarh 160 012, India.
Email: [email protected]
|
Gastrointestinal obstruction in children may be due to a variety of
conditions. 150 cases of acute intestinal obstructions seen over a
period of 180 months were reviewed. Intestinal atresia was the comonest
cause (34, 22.4%).
Keywords: Intestinal obstruction, Neonates, India.
|
|
Gastrointestinal obstruction in the pediatric age group may be due to a
variety of congenital and acquired conditions. Over a period of 18 months;
150 cases of acute intestinal obstructions accounted for 40% of the
abdominal emergencies at our center. Children with esophageal atresia,
anorectal ano-malies, Hirschsprung’s disease, adhesive intestinal
obstruction not requiring surgery, and peritonitis without mechanical
obstruction were excluded.
Seventy eight percent (118) were males and 32(22%) were
females (M: F: 3.6:1). The children aged between 1-12 months constituted
42% (n=63) of the patients and 35% (n=53) were neonates.
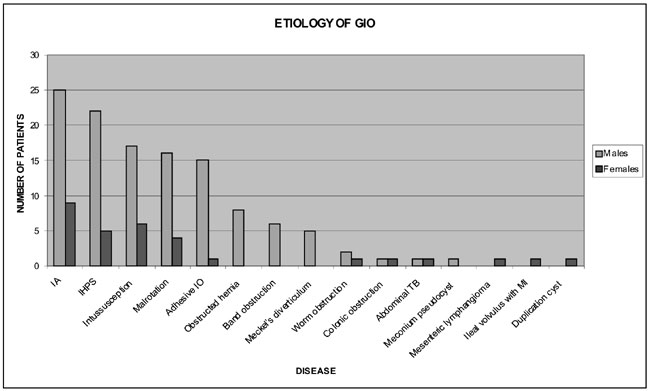
Etiological distribution of the cases is shown in
Fig.1. Intestinal atresias were the commonest and accounted for
22.4% (n=34) of the cases. Malrotation (n=11), congenital
band obstruction (n=3), meconium pseudocyst (n=2),
Obstructed hernia (n=1), duplication cyst jejunum (n=1) and
infantile hypertrophic pyloric stenosis (n=1) were other causes of
obstruction in neonates. Out of 23 (15%) patients of intussusception,
18(76%) were between 6 month to 1 year of age and only 59%(16) of the
patients had bleeding per rectum. Pathological lead point (PLP) was seen
in 4 (19%) patients of ileocolic intussusception. Of the 20 patients of
malrotation, 11 (55%) were less than one month old, 5(25%) between 1 month
and 1year and 4 (20%) were 1 to 6 years.
 |
|
Fig. 1 Distribution of etiology of
gastrointestinal obstruction in children. |
Many studies in Western and South African countries
show similar etiological prevalence as in our institute(1-3). However,
there were several differences observed in the presentations in different
groups of GIO as compared to the classical descriptions(1,4,5).
Intussusception occurred below 1year of age in 76%(18) of our patients and
PLP was present in 19% of them, unlike the previous reports in the
literature. Bleeding per rectum was seen in 59% of the patients only,
compared to a higher incidence reported by others. Fifty five percent of
our patients presented with malrotation in the neonatal period, in
contrast to 75% neonatal presentations described in the literature. The
intestinal obstruction in malrotation may be waxing and waning type and
requires a high index of suspicion so as not to miss the diagnosis.
References
1. Ameh EA, Chirdan LB. Neonatal intestinal obstruction
in Zaria, Nigeria.East Afr Med J 2000; 77: 510-513.
2. Rescorla FJ, Grosfeld JL. Intestinal atresia and
stenosis: Analysis of survival in 120 cases. Surgery 1985; 98: 668-676.
3. DallaVecchia LK, Grosfeld JL, West KW, Rescorla FJ,
Scherer LR, Engum SA. Intestinal atresia and stenosis: a 25-year
experience with 277 cases. Arch Surg 1998; 133: 490-497.
4. Adejuyigbe O, Fashakin EO. Acute intestinal
obstruction in Nigerian children. Trop Gastroenterol 1989; 10: 33-40.
5. Olumide F, Adedeji A, Adesika AO. Intestinal obstruction in Nigerian
children: J Pediatr Surg 1976; 11: 195-204.
|
|
|
 |
|
